
Author Contributions
Copyright © 2021 M. Elqatni, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
A45-year-old man, with no prior pathologic antecedent was admitted to the internal medicine department for a 3weeks history of abdominal pain. This symptom occurred in the context of apyrexia and 4 kilogram weight loss. Abdominal examination was a painful abdomen, distended. The skin examination noted painful genital andoral ulcers with pustlar lesions in the back. Angio CT scan revealed an aneurysm of the right common iliac artery (Figure 1).Artégraphie the lesion showed the same described above, showing the saccular aneurysm (Figure 2). He had no other aneurysmal localizations.
Figure 1.Angio CT scan revealed an aneurysm of the right common iliac artery.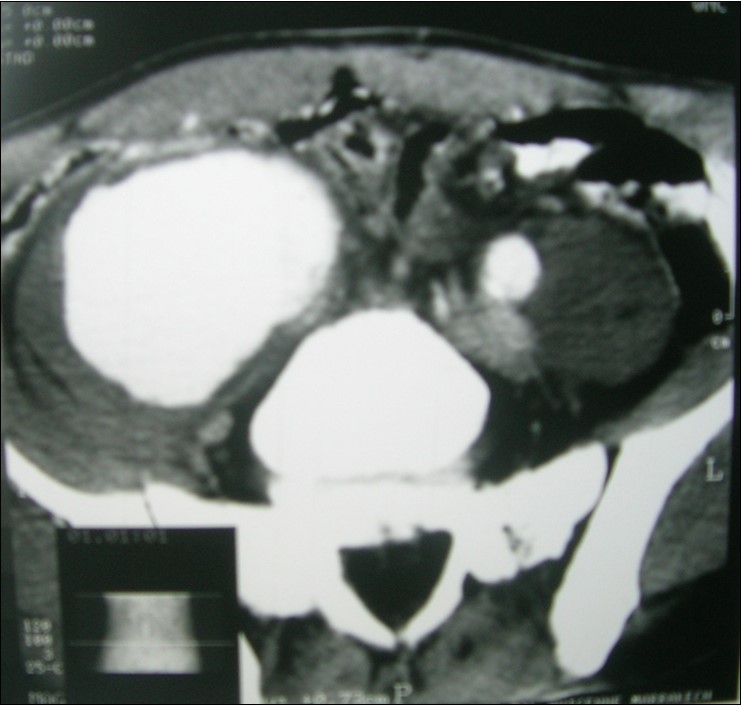
Figure 2.Artégraphie showed the saccular aneurysm.
Laboratory tests found inflammatory. The infectious analysis (VDRL-TPHA, Mycobacteria) was negative. HLA-B51 was positive. The diagnosis of Behçet’s disease was made. The patient was treated surgically with a prosthetic iliac-femoral, cyclophosphamide and methylprednisolone pulses relayed by oralprednisone 1 mg/kg/j.
Orogenital aphthosis, skin lesions and uveitis characterize Behçet’s disease (BD)1. The incidence of cardiovascular complications in BD is approximately 30%, although these complications are apparently the major cause of death, which highlights the gravity of the condition. Of the vascular lesions reported, 25% affect the venous system exclusively and 7% the arterial system exclusively, 68% of the patients with vascular involvement have both
types 2.