Abstract
Introduction:
Cemento-ossifying fibroma is is a reactive lesion arising from the soft tissues (gingiva).
Case report:
A 13-year-old boy presented with the complaint of lump in mandibular right posterior region on the lingual side since a month. The patient presented no symptoms and had no medical history of interest. The lesion was excised and submitted for histopathological evaluation, which gave a diagnosis of peripheral cemento-ossifying fibroma.
Discussion:
Periheral Cemento-ossifying fibromas are slow-growing lesions, and are more frequent in women between the second and third decades of life. Although the underlying cause is not known, there have been reports of the lesion developing after irritation/ trauma in the concerned area. Due to the good delimitation of the tumor, surgical removal and curettage is the treatment of choice.
Author Contributions
Academic Editor: Fernanda Goncalves Salum, University of Rio
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Jaai Rane, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction:
Peripheral cement ossifying fibroma (PCOF) accounts for 3.1 % of all oral tumors and for 9.6% of gingival lesions.1, 2 Due to their clinical and histopathological similarities, some PCOFs are believed to develop initially as a pyogenic granuloma that undergoes fibrous maturation and subsequent calcification. The mineralized product originates from periosteal cells or from the periodontal ligament.3
In 1872, Menzel gave the first description of a variant of ossifying fibroma, calling it a cemento-ossifying fibroma, in a 35-year-old woman with a long-standing large tumor of the mandible.4Gardner(1982)recommended that the term PCOF be used to describe a common, non-neoplastic lesion that shows histopathological characteristics of a fibrous cellularized stroma containing a variety of mineralized material, differentiating it from peripheral odontogenic fibroma which is characterized by odontogenic epithelium and dysplastic dentin.5
Case Report:
A 13year-old male patient reported to the Department of Pediatric and Preventive Dentistry with a chief complaint of the presence of a ‘lump’ in the lower right back region. The history revealed that the patient had buccal abscess in relation to 85 two months back for three days which reduced on medications. The tooth (85) exfoliated within 1 month and soon after the exfoliation, patient noticed a lump in that region. The lump was painless and increased in size in the last one month. Patient experienced discomfort in speech since the last one week. No abnormality or asymmetry was noted on extra-oral examination. Intraoral clinical examination revealed a painless, fibrous nodular mass with a sessile base in the right lower gingival margin extending from the mesial surface of 44 to distal surface of 45 on the lingual surface, measuring approximately 2 cm in diameter and showing a rough surface and color similar to that of the adjacent mucosa(Figure 1)
Figure 1.Pre operative size and extent of lesion
Depending on the history, clinical and radiographic examination, a provisional diagnosis of Gingival enlargement was made. The treatment planned was surgical excision of the lesion with laser 1 week later on the next visit.
Figure 2.Excised lesion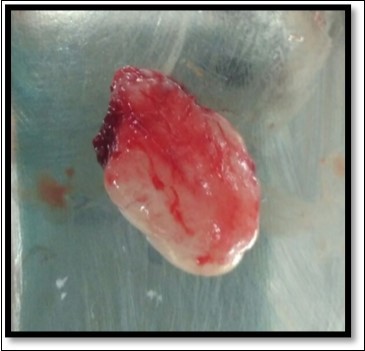
During the next visit local anesthesia was given. The lesion was excised with the help of soft tissue laser and sent for histological examination. (Figure 2) Histological report confirmed the lesion is Peripheral cemento-ossifying Fibroma. Histological analysis showed lesional tissue comprising of both trabecular bone and woven bone. Periphery of the lesion showed numerous globular and irregular cementum like calcification. In most areas these calcification coalesced with each other forming bigger calcification. The supporting connective tissue stroma was loose fibrillar with less cellularity. Detached overlying parakeratinized epithelium was observed in one area. (Figure 3) Post operative evaluation revealed normal healing after one month. (Figure 4)
Figure 3.Histologically H & E stained section shows trabecular bone and woven bone more towards the center of the lesion
Figure 4.One month follow-up
Discussion:
Cemento-ossifying fibroma is a reactive lesion arising from the soft tissues.6 It is a slow-growing lesion most often seen in women between the third and fourth decades of life.
It may occur at any age range, but exhibits a peak incidence between the second7 and third decade.8 The prevalence of this lesion has been reported to be 1.9% in children aged 0 to 9 years, 10% in 5 to 9 years with peak prevalence between 10 and 19 years.1, 9, 10
Etiology of this lesion is often associated with local irritants and constant irritation present during exfoliation of the deciduous teeth and eruption of the permanent teeth may result in an increased incidence of reactive lesions which originate from the periodontal ligament11 as it was seen in our case. Hormonal influences may play a role too, as the lesions have shown a female predilection, with increasing occurrence in the second decade of age and declining incidence after the third decade.12
Clinically, PCOF manifests as a pedunculated or sessile nodular mass, which usually originates in the interdental papilla. Its color is similar to that of the mucosa unless the lesion is ulcerated.11 In the present case it was noted that the adjacent tooth was displaced. Most tumors measure less than 2 cm in diameter, although lesions larger than 10 cm are occasionally observed. In the present case, the lesion was ovoid in shape measuring about 2x1x1 cm in dimensions. About 60% of the tumors occur in the maxilla with more than 50% affecting the incisor and canine region.11
Histologically, PCOF shows a parakeratinized and hyperplastic epithelium and well-cellularized connective tissue containing mineralized components ranging from bone to cementum and, less frequently, dystrophic calcifications.11 Histopathological examination is essential to confirm the diagnosis of PCOF, since clinically it resembles a pregnancy tumor, epulis fibrosa, inflammatory hyperplasia, or peripheral and central giant cell granuloma.3
The differential diagnosis with pyogenic granuloma is common. Pyogenic granuloma is the initial lesion of gingiva which occurs due to chronic irritation in the gingival sulcus whereas peripheral ossifying fibroma occurs as a sequelae to pyogenic granuloma when fibrous maturation and calcification occurs.
Due to the good delimitation of the tumor, surgical removal and curettage is the treatment of choice. The prognosis is usually good.6 Recurrence is more common if the base of lesion remains, repeated injury, and/or the persistence of the local irritants. The rate of recurrence has been reported to vary from 8.9% to 20%. The average time interval for the first recurrence is 12 months.1, 7, 12 Therefore, regular follow-up is required. In the present case also, our patient is under follow-up. Any irritant etiological factor such as calculus, an ill-adapted orthodontic appliance or poor restorations should be removed. Extraction of adjacent teeth is rarely required in the early stages of the tumor. Recurrence of the lesion due to incomplete surgical removal along with the presence of local irritating factors has been reported.12
Conclusion:
PCOF is a slowly progressive lesion generally with limited growth. Many cases will progress for long periods before the patient seeks treatment because of lack of symptoms associated with the lesion. It is possible to misdiagnose PCOF from other reactive lesions arising from the gingiva. Therefore, histopathological examination is essential for an accurate diagnosis and for proper management.
References
- 1.Kenney J N, Kaugars G E, Abbey L M.Comparison between the peripheral ossifying fibroma and peripheral odontogenic fibroma. , J Oral Maxillofac Surg1989;47: 378-382.
- 2.Walters J D, Will J K, Hatfield R D, Cacchillo D A, Raabe D A.Excision and repair of the peripheral ossifying fibroma: a report of 3 cases. , J Periodontol2001;72: 939-944.
- 4.H G Sarwar, M K Jindal, Ahmad S S. (2008) Cemento-ossifying fibroma-a rare case. , J Indian Soc Pedod Prev Dent2008; 26, 128-31.
- 5.Gardner D G.The peripheral odontogenic fibroma: An attempt to classification. Oral Surg Oral Med Oral Pathol 1982;54:. 40-48.
- 6.Silvestre-Rangil J, Silvestre F J, Requeni-Bernal J. (2011) Cemento-ossifying fi- broma of the mandible: Presentation of a case and review of the literature. , J Clin Exp Dent.; 3(1), 66-9.
- 7.Das S, Das A K.A review of pediatric oral biopsies from a surgical pathology service in a dental school. Pediatr Dent1993;15:. 208-211.
- 8.Bodner L, Dayan D. (1987) Growth potential of peripheral ossifying fibroma. , J Clin Periodontol1987; 14, 551-554.
- 9.ZES Cuisia, Brannon R B. (2001) Peripheral ossifying fibroma – a clinical evaluation of 134 pediatric cases. Pediatr Dent2001;. 23, 245-248.