
Abstract
Evidence shows that depressive symptoms are associated with faster progression to AIDS in HIV-infected populations. Physical symptoms, self-esteem, and emotional support have been reported to play a major role in contributing to depressive symptoms. However, comparisons of different sources of support—specifically family vs. friends— have only been made in a few previous HIV studies. Therefore, the objectives of this study among HIV-positive perinatal Thai women were to examine: 1) both the direct and indirect effects of physical symptoms and emotional support on depressive symptoms; 2) which source of support is more significant, family or friends; and 3) the direct effect of self-esteem on depressive symptoms. Results revealed that half of the participants experienced major depressive symptoms. Physical symptoms and self-esteem both had direct effects on depressive symptoms. Emotional support, from friends and family, had an indirect effect on depressive symptoms. Treating physical symptoms and increasing self-esteem through emotional support, could help decrease depressive symptoms in the target population. Finally, it is crucial that routine screening for depressive symptoms is established at all HIV clinics for perinatal women in Thailand.
Author Contributions
Academic Editor: Koosha Paydary, (SSRC) and Iranian Research Center for HIV/AIDS (IRCHA), TUMS
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2014 Ratchneewan Ross, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
At the end of 2009, the Joint United Nations Programme on HIV/AIDS1 estimated that 33.3 million people were living with HIV, including at least 600,000 Thai adults (ages 15–49 years), 20,000 of whom were pregnant women2. In general, HIV infections cause greater problems in developing countries such as Thailand than in developed countries, partly because of a lack of antiretroviral medications. Studies have shown that depressive symptoms are associated with non-adherence to antiretroviral treatment 3, 4, 5 faster disease progression,5, 6, 7 and poorer quality of life.8
Among HIV-positive perinatal women, being single, having a low income, having a low level of education, being younger, and being unemployed are often found to be correlated with depressive symptoms.9, 10, 11, 12, 13 Other factors affecting depressive symptoms in those who are HIV positive include presence of physical symptoms, low emotional support, low self-esteem, and poor physical health.11, 12, 14, 15, 16, 17, 18, 19
Studies in various countries have found that HIV-positive perinatal women with low self-esteem tend to report more depressive symptoms than those with high self-esteem.11, 12, 17, 20 Qualitative studies have found that HIV-positive pregnant women in Thailand with low self-esteem are more likely to be depressed than those with high self-esteem, and stigmatization related to the infection seemed to be an antecedent of low self-esteem.21, 22, 23 Further, perinatal women with HIV tend to have low self-esteem and negative personal perceptions that lead to depression. They consider themselves as inferior or incapable women and fear being condemned both on a moral level and for having failed as mothers.24 Studies have found that HIV-positive pregnant and postpartum Thai women worry constantly about their infant's health, fearing that the fetus/infant has been infected.22, 25, 26 Negative perceptions about the infant's health can compound the mother's negative feelings of being incompetent and have been positively linked to depressive symptoms in Thai and U.S. postpartum women.12, 27
Emotional support also plays a major role in contributing to depressive symptoms. In Thailand, emotional support from family and friends has been negatively related to depressive symptoms in postpartum women28, 29 and HIV-positive pregnant women.11 However, to our knowledge, the two sources of support have not been compared in most previous HIV studies,12, 14, 15, 16, 18 except in one study among HIV-positive women19and youth in the USA.30 Family support was found to be related to less depression among young US individuals.30 With only limited support, HIV-positive individuals are more likely to exhibit depressive symptoms.11, 21, 22, 31 Other correlates of depressive symptoms include a history of psychiatric disorders,32, 33 low income,34 and low levels of education.35
The objectives of this study were to examine among HIV-positive perinatal Thai women: 1) both the direct and indirect effects of physical symptoms and emotional support on depressive symptoms; 2) which source of support is more significant, family or friends; and 3) the direct effect of self-esteem on depressive symptoms. We hypothesized that physical symptoms and emotional support had both direct and indirect effects on depressive symptoms, while self-esteem had a direct effect on depressive symptoms (Figure 1). We also hypothesized that family is a stronger source of support than friends in the target population.
Figure 1.The initial/hypothesized path model with combined family & friend support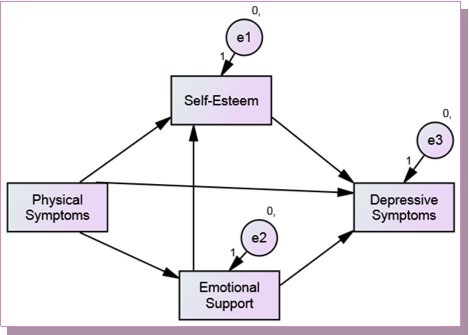
Materials and Methods
Data were combined from two separate previous studies that specifically examined only the direct effects of predictors of depressive symptoms among HIV-positive pregnant (n = 127) and postpartum women (n=85) in four hospitals in Thailand.11, 12 Both studies included pregnant or postpartum adult women who were diagnosed with an HIV infection and who could read and write in Thai. The exclusion criteria for both studies included a history of depression/psychosis and substance abuse. The participants from both studies were comparable regarding their demographic-socioeconomic status (e.g., age, number of children, marital status, income), based on either the Chi-square or independent t-test. The study protocols were approved by five internal review boards before data collection which took place between 2004 and 2007. A questionnaire packet was administered at one of the hospital’s private rooms. Well-established Likert-type scales with back translation were used to measure three key study variables. The 20-item Center for Epidemiologic Studies Depression Scale CES,36 was used to measure depressive symptoms (α=.91), the 12-item Multidimensional Scale of Perceived Social Support MSPSS37, 38 to measure combined emotional support from family and friends (α=.87), the 8-item family subscale of the MSPSS to measure family support (α=.87), the 4-item friend subscale of the MSPSS to measure friend support (α=.85), and the 10-item Rosenberg Self-esteem scale R39 to measure self-esteem (α=.78). The higher the CES-D, MSPSS, and R-SE scores, the more depressive symptoms, the more emotional support, and the more self-esteem, respectively. Physical symptoms were measured with two questions. The first question asked if the woman had experienced any physical symptoms in the past seven days with possible answers of yes (1) or no (0). If the answer was yes, the woman was asked to rate the extent to which the symptom(s) interfered with her daily activities with possible responses ranging from “Not at all” (0) to “A lot” (3). The scores from these two items were summed up to create a total score which ranged from 0 to 4. The alpha for this measure was 0.74.
Using SPSS version 20, key variables were screened for multivariate outliers (using Mahalonobis distance), multicollinearity (using Variance Inflation Factor), and normality, linearity, & homoscedasticity (using plots of regression standardized residuals and predicted values). No problems were detected.40An initial path analysis was constructed and run to examine the relationships among physical symptoms, combined emotional support, self-esteem, and depressive symptoms using maximum likelihood estimates through AMOS version 21 (Figure 1).
Results
The average age of the participants was 26.4 (SD=5.4) with each averaging one child per family. Approximately half of the participants were unemployed (45%), most lived with their spouse (90%), and more than half reported they did not make enough money (62%). About half of the participants had known their HIV status for over 6 months. Three out of four (75.5%) reported no physical symptoms. The top three frequent symptoms reported included fatigue (n=32), anemia (n=27), and weight loss (n=15). Table 1 shows each key variable’s mean, standard deviation, total score, and possible score range.
Table 1. Mean, standard deviation, and total score of key variables (n=212)| Variable | Mean | (SD) | Score | Possible Range |
| Self-esteemEmotional Support | 29.459.3 | 3.5611.50 | 19-4012-84 | 10-4012-84 |
| Physical symptomsDepressive symptoms | 0.6823.0 | 1.3010.54 | 0-4 2-51 | 0-40-60 |
As based on Radloff’s (1977) cutoff recommendation,36 one out of four (24.6%) did not experience depressive symptoms (CES-D score <16), while another one out of four (25.6%) reported minor depressive symptoms (CES-D score ≥16 but <23). Importantly, about half of all participants (49.8%) reported major depressive symptoms (CES-D score ≥ 23).
Table 2 shows results of the hypothesized/initial model (with combined emotional support from family and friends) which include unstandardized path coefficients with their respective standard errors, critical ratios, p-values, standardized path coefficients, and disturbance variances. Figure 2 shows that depressive symptoms were predicted by physical symptoms, combined emotional support from family and friends, and self-esteem which together accounted for 32% (R2 = .32) of the explained variance in depressive symptoms. Significant standardized direct, indirect, and total effects are presented in Table 3 for this model and the other models which will follow. Table 4 shows values of model fit indices for this model and other models which also will follow. The path coefficients from physical symptoms to self-esteem, from physical symptoms to combined emotional support, and from combined emotional support to depression were not significant (Figure 2). Therefore, the model was trimmed by excluding non-significant paths and reanalyzed.
Table 2. Maximum likelihood estimates for the recursive hypothesized path model (family & friends support) (Also see Figure 2)| Parameter | Unstandardized | SE | CR | p | Standardized | ||
| Emotional support | <--- | Physical symptoms | -1.191 | 1.318 | -.903 | .366 | -.079 |
| Self-esteem | <--- | Emotional support | .009 | .002 | 4.500 | *** | .299 |
| Self-esteem | <--- | Physical symptoms | -.052 | .039 | -1.321 | .187 | -.110 |
| Depressive symptoms | <--- | Self-esteem | -13.569 | 1.831 | -7.412 | *** | -.460 |
| Depressive symptoms | <--- | Physical symptoms | 3.117 | 1.001 | 3.113 | .002 | .225 |
| Depressive symptoms | <--- | Emotional support | -.078 | .057 | -1.382 | .167 | -.085 |
| Disturbance/Residual variances | |||||||
| Emotional support | 130.792 | 12.935 | |||||
| Self-esteem | .114 | .011 | |||||
| Depressive symptoms | 75.134 | 7.711 | |||||
Figure 2.Results of the initial path model with combined family & friend support (R2 values are shaded) Note: ns = non-significant
| Model | Direct effect: from → to | Indirect effect from emotional support → self-esteem → depressive symptoms | Total effect for depressive symptoms | R2 | ||
| Physical symptoms→ Depressive symptoms | Emotional support→ Self-esteem | Self-esteem→Depressive symptoms | ||||
| 1 Initial: Combined family & friend support (Figure 2) | .22 | .30 | -.46 | -.14 | -.38 | .32 |
| 2 Trimmed: Combined family & friend support (Figure 3) | .23 | .31 | -.50 | -.15 | -.42 | .31 |
| 3 Trimmed: Friend support (Figure 4) | .23 | .20 | -.50 | -.15 | -.42 | .31 |
| 4 Trimmed: Family support (Figure 5) | .23 | .30 | -.50 | -.15 | -.42 | .30 |
| Model | Chi-square | CFI | IFI | NFI | RMSEA | LO90 | HI90 | Note | ||
| Value | df | p | ||||||||
| 1 Initial: Combined family & friend support (Figure 2) | 0 | 0 | - | 1.0 | 1.0 | 1.0 | .206 | .172 | .244 | Just-identified model |
| 2 Trimmed: Combined family & friend support (Figure 3) | 1.86 | 2 | .173 | .990 | .991 | .981 | .065 | .000 | .210 | Second best model fit |
| 3 Trimmed: Friend support (Figure 4) | 6.32 | 2 | .042 | .946 | .951 | .930 | .102 | .017 | .197 | Least model fit |
| 4 Trimmed: Family support (Figure 5) | 2.71 | 2 | .26 | .992 | .992 | .971 | .041 | .000 | .151 | Best model fit |
Table 5 shows maximum likelihood results of the trimmed model (with combined emotional support). Figure 3 shows a non-significant covariance between physical symptoms and family and friend support. The model fits the data well and better than the initial model, based on various model fit indices. From Table 4, the Chi-square value was not significant. The values of the Comparative Fit Index (CFI), Incremental Fit Index (IFI), and Normed Fit Index (NFI) were larger than .95, which indicate a good fit between the model and the data.41, 42Moreover, the Root Mean Squared Error of Approximation (RMSEA) was less than .80.41 The confidence interval of RMSEA is wide, indicating possible estimate instability.41 The R2 value of .31 for depressive symptoms in the trimmed model wasslightly smaller than that of the initial model. Statistically, physical symptoms had a positive direct effect on depressive symptoms, while self-esteem had a negative direct effect on depressive symptoms (Figure 3). Combined emotional support had no direct effect but did have an indirect effect on depressive symptoms through self-esteem (Table 3). Table 5 shows the maximum likelihood estimates of the trimmed path model with combined emotional support from family and friends.
Table 5. Maximum likelihood estimates for the recursive trimmed path model (family & friends support) (Also see Figure 3)| Parameter | Unstandardized | SE | CR | p | Standardized | ||
| Self-esteem | <--- | Emotional support | .010 | .002 | 4.640 | *** | .308 |
| Depressive symptoms | <--- | Self-esteem | -14.554 | 1.723 | -8.445 | *** | -.498 |
| Depressive symptoms | <--- | Physical symptoms | 3.104 | .995 | 3.118 | .002 | .226 |
| Depressive symptoms | <--- | Emotional support | -.074 | .057 | -1.295 | .195 | -.081 |
| Disturbance/Residual variances | |||||||
| Self-esteem | .116 | .011 | 10.149 | *** | |||
| Depressive symptoms | 76.025 | 7.798 | 9.749 | *** | |||
Figure 3.Results of the trimmed path model with combined family & friend support (R2 values are shaded)
To examine the effect of family support vs. friend support, we ran two models separately—one with friend support and the other one with family support. Table 6 shows the friend support model’s unstandardized path coefficients with their respective standard errors, critical ratios, p-values, standardized.path coefficients, and disturbance variances. Figure 4 shows a non-significant covariance between physical symptoms and family and friend support. Statistically, physical symptoms had a positive direct effect on depressive symptoms, while self-esteem had a negative direct effect on depressive symptoms. Friend support had no direct effect but did have an indirect effect on depressive symptoms through self-esteem (Figure 4) (Table 3). This friend support model was found to fit the data less well than the combined support model, based on different model fit indices (Table 4). The R2 value of .31 for depressive symptoms in this model wasslightly smaller than that of the initial model.
Table 6. Maximum likelihood estimates for the recursive path model (friend support) (Also see Figure 4)| Parameter | Unstandardized | SE | CR | p | Standardized | ||
| Self-esteem | <--- | Emotional support | .025 | .006 | 4.464 | *** | .297 |
| Depressive symptoms | <--- | Self-esteem | -14.572 | 1.722 | -8.461 | *** | -.499 |
| Depressive symptoms | <--- | Physical symptoms | 3.106 | .996 | 3.117 | .002 | .226 |
| Disturbance/Residual variances | |||||||
| Self-esteem | .117 | .012 | 10.149 | *** | |||
| Depressive symptoms | 76.013 | 7.801 | 9.744 | *** | |||
Figure 4.Results of friend support path model (R2 values are shaded)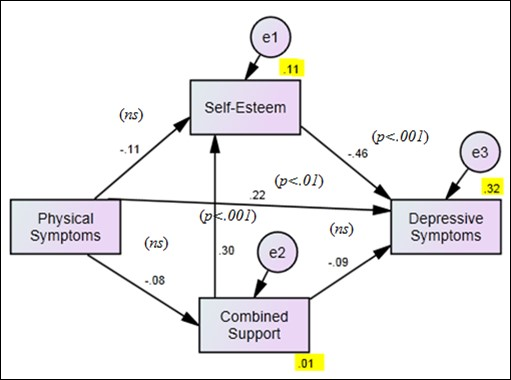
Table 7 shows the family support model’s maximum likelihood results. Figure 5 shows a non-significant covariance between physical symptoms and family and friend support. The model fits the data best among all four models, based on various model fit indices (Table 4). The R2 value of .30 for depressive symptoms in this model wasslightly smaller than that of the initial, trimmed, and friend support models. Statistically, physical symptoms had a positive direct effect on depressive symptoms, while self-esteem had a negative direct effect on depressive symptoms. Family support had no direct effect but did have an indirect effect on depressive symptoms through self-esteem (Figure 5). Again, Table 3 summarizes the significant standardized direct, indirect, and total effects, and R2 values in depressive symptoms for all of the four models.
Table 7. Maximum likelihood estimates for the recursive path model (family support) (Also see Figure 5)| Parameter | Unstandardized | SE | CR | p | Standardized | ||
| Self-esteem | <--- | Emotional support | .013 | .003 | 4.464 | *** | .297 |
| Depressive symptoms | <--- | Self-esteem | -14.572 | 1.722 | -8.461 | *** | -.499 |
| Depressive symptoms | <--- | Physical symptoms | 3.106 | .996 | 3.117 | .002 | .226 |
| Disturbance/Residual variances | |||||||
| Self-esteem | .117 | .012 | 10.149 | *** | |||
| Depressive symptoms | 76.013 | 7.801 | 9.744 | *** | |||
Figure 5.Results of family support path model (R2 values are shaded)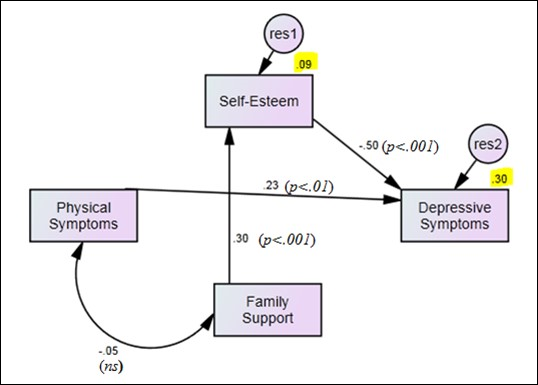
Discussion
This study is the first to examine both the direct and indirect effects of physical symptoms and emotional support on depressive symptoms among pregnant and postpartum women in Thailand. We found that about half of our 212 HIV-infected pregnant and postpartum participants reported major depressive symptoms, based on Radloff’s (1977) CES-D cutoff score of ≥ 23.36 This depression rate is comparable to those in previous studies among HIV-positive perinatal women around the world: 47% in pregnant women17and 42.2% in postpartum women in South Africa,43 53%, in pregnant US women,33 30.8% in perinatal US women,44 and 54% in postpartum women in Zimbabwe.45Based on this high prevalence of depression rates, we recommend that all HIV clinics in Thailand do a routine screening of HIV-positive pregnant and postpartum women. An early detection of clinical depression is crucial so that appropriate treatment and care can help to delay progress to full blown AIDS in depressed HIV-positive perinatal women.
Results from our trimmed path model with the combined family and friend support showed that the data fit the model well, based on various model fit indices. Among our perinatal HIV-positive Thai women, physical symptoms had a positive direct effect on depressive symptoms, meaning that the more physical symptoms our participants experienced, the more depressed they were. Frequently, reported symptoms among our participants included fatigue, anemia, and weight loss. Detecting such physical symptoms and providing appropriate care and treatment to reduce the symptoms may help lessen depressive symptoms. Generally, in previous research, fatigue was found to be moderately associated with depressive symptoms among HIV-positive individuals, and more so among females than males.46, 47 We noted that even though fatigue is correlated to depressive symptoms, it has its unique contribution to negative physical functions. Thus, fatigue is a separate concept and needs to be assessed separately from depressive symptoms and should be treated when detected.48, 49
No indirect effect from physical symptoms was found either through emotional support (combined family and friends) or through self-esteem leading to depressive symptoms. However, combined emotional support positively affected self-esteem, and self-esteem had a negative direct effect on depressive symptoms—indicating that combined emotional support had an indirect effect on depressive symptoms through self-esteem. In other words, the more combined emotional support from family and friends our participants received, the higher their self-esteem, and the fewer depressive symptoms they experienced. Our results are consistent with those from previous studies among HIV-positive individuals in different countries (e.g., Brazil, India, South Africa, Thailand, and the USA) in that self-esteem is directly correlated with depression.11, 12, 15, 17, 50
A question arises: “How can self-esteem be strengthened in HIV-positive perinatal women in Thailand?” The result in our trimmed model suggests that combined emotional support is a significant and helpful way to increase self-esteem among our target population. Combined emotional support in our study involved support from two sources: family and friends. Which source of support is more helpful? To answer this question, we analyzed family support and friend support separately. Our results revealed that family support is just as important as that of friends. These results are different from those of a previous study conducted among HIV-positive US women which revealed that support from friends was more positive than from family.19This inconsistency could be explained in light of cultural differences. While family in the USA values individuality, in Thailand a family is considered as “oneness”—meaning that both immediate and extended family members belong to one family.51Thus, in Thailand, when any family member is affected by a disease or any unfortunate event, every member is in the overall family structure expected to help out emotionally, tangibly, and/or informationally.51In this regard, it is not surprising that family support was found to be just as helpful as friend support in our Thai study.
If the HIV-positive perinatal woman does not have a family, having a friend who understands her and helps her feel good about herself is indeed valuable. If both support from family and friends are available, both sources of support should be encouraged by health care professionals to help HIV-positive perinatal women in Thailand feel loved and included—thereby increasing their self-esteem and decreasing their depressive symptoms. Such support coincides with Leary’s notion that “self-esteem system is an internal, psychological gauge that monitors the degree to which the individual is being included versus excluded by other people. Self-esteem, then, is an internal representation of social acceptance and rejection.” 52 Thus, including family and/or friend support in counseling services for Thai HIV-positive perinatal women will be beneficial.
Our research, nevertheless, is limited in that only quantitative data were available, and the study is correlational in nature. Future research should include both quantitative and qualitative data collection (mixed methods) so that the cultural context and the processes of emotional support, self-esteem, and depressive symptoms can be examined in more depth. A longitudinal study with mixed methods methodology will maximize the results’ validity and deepen our understanding of the phenomenon of depressive symptoms among HIV-positive perinatal women in Thailand. A larger sample size for future studies will also be helpful because the confidence intervals around RMSEA in our study indicate possible result instability. Finally, comparing the effects of family vs. friend support on self-esteem and depressive symptoms among HIV-positive perinatal women in other cultures beyond the Thai and US cultures will be helpful.
Conclusion
Strong evidence in the literature shows that depressive symptoms are associated with faster progression to AIDS in HIV-infected populations. Results in this study revealed that half of the participants experienced major depressive symptoms. It is crucial that routine screening for depressive symptoms is established at all HIV clinics for perinatal women in Thailand. Physical symptoms and self-esteem had direct effects on depressive symptoms. Therefore, treating physical symptoms and increasing self-esteem through emotional support - especially family and friends support - could decrease depressive symptoms in the target population. Educating family and health care professionals about a potential positive effect of emotional support from family and friends may encourage more emotional support endeavors and may be particularly beneficial for HIV-positive pregnant and postpartum Thai women.
References
- 1. (2011) . Joint United Nations Programme on HIV/AIDS.Thailand:AIDS info.Retrieved from http://www.unaids.org/en/regionscountries/countries/thailand/
- 2. (2010) Thai Red Cross Society.The Thai Red Cross AIDS. research center.Retrieved from: http://english.redcross.or.th/content/page/954
- 3.Byakika-Tusiime J, Crane J, Oyugi J, Ragland K, Kawuma A.Longitudinal antiretroviral adherence in HIV+ Ugandan parents and their children initiating HAART in the MTCT-plus family treatment model: role of depression in declining adherence over time. doi: 10.1007/s10461-009-9546-x. AIDS and Behavior.
- 4.Structural Equation Model of HIV-Related Stigma, Depressive Symptoms, and Medication Adherence. , AIDS & Behavior doi:, 10-1007.
- 5.I Sumari-de Boer, Sprangers M, Prins J, Nieuwkerk P. (2012) HIV stigma and depressive symptoms are related to adherence and virology response to antiretroviral treatment among immigrant and indigenous HIV infected patients. , AIDS and Behavior 16(6), 1681-1689.
- 6.Alciati A, Gallo L, Monforte A, Brambilla F, Mellado C. (2007) Major depression-related immunological changes and combination antiretroviral therapy in HIV-seropositive patients. Human Psychopharmacology: Clinical &. , Experimental 22(1), 33-40.
- 7.Antelman G, Kaaya S, Ruilan W, Mbwambo J, Msamanga G I. (2007) . Depressive Symptoms Increase Risk of HIV Disease Progression and Mortality Among Women in Tanzania. Journal of Acquired Immune Deficiency Syndromes 44(4), 470-477.
- 8.Adewuya A, Afolabi M, Ola B, Ogundele O, Ajibare A. (2008) Relationship between depression and quality of life in persons with HIV infection in Nigeria. , International Journal of Psychiatry In Medicine 38(1), 43-51.
- 9.Beck C. (2002) Revision of the Postpartum Depression Predictors Inventory. , Journal of Obstetric, Gynecologic & Neonatal Nursing 31(4), 394-402.
- 10.Gupta R, Dandu M, Packel L, Rutherford G, Leiter K. (2010) Depression and HIV in Botswana: a population-based study on gender-specific socioeconomic and behavioral correlates. , PloS one 5(12), 1425.
- 11.Ross R, Sawatphanit W, Zeller R.Depressive symptoms among HIV-positive pregnant women in Thailand. , Journal of Nursing Scholarship doi:, 10-1111.
- 12.Ross R, Sawatphanit W, Mizuno M, Takeo K.Depressive symptoms among HIV-positive postpartum women in Thailand. doi: 10.1016/j.apnu.2010.05.003. Archives of Psychiatric Nursing.
- 13.Unnikrishnan B B, V, Ramapuram J T, Hegde S S. (2012) Study of depression and its associated factors among women living with. HIV AIDS in coastal South India. Retrovirology 10-1186.
- 14.Jia H, Uphold C, Wu S, Reid K, Findley K. (2004) Health-related quality of life among men with HIV infection: effects of social support, coping, and depression. , AIDS Patient Care & STDs 18(10), 594-603.
- 15.Jagannath V, Unnikrishnan B, Hegde S, Ramapuram J, Rao S.(December2011) Association of depression with social support and self-esteem among HIV positives. doi: 10.1016/j.ajp.2011.10.006. , Asian Journal of Psychiatry
- 16.Li L, Lee S, Thammawijaya P, Jiraphongsa C, Rotheram-Borus M.(August2009) Stigma, social support, and depression among people living with HIV in Thailand. , AIDS Care doi:, 10-1080.
- 17.Makin J D. (2010) Depression scores in a cohort of HIV positive women followed from diagnosis during pregnancy to eighteen months postpartum:A master’s thesis,theUniversityofPretoria,SouthAfrica.
- 18.Mosack K, Weinhardt L, Kelly J, Gore-Felton C, McAuliffe T. (2009) Influence of coping, social support, and depression on subjective health status among HIV-positive adults with different sexual identities. , Behavioral Medicine 34(4), 133-144.
- 19.Serovich J M, Kimberly J A, Mosack K E, Lewis T L. (2001) The role of family and friend social support in reducing emotional distress among HIV-positive women.doi: 10.1080/09540120120043982.AIDS Care.
- 20.Wang S-Y, Jiang X-Y, Jan W-C, Chen C-H. (2003) A comparative study of postnatal depression and its predictors in Taiwan and mainland China. , American Journal of Obstetrics 189(5), 1407-1412.
- 21.Ross R, Sawatphanit W, Suwansujarid T, Draucker C B. (2007) Life story of and depression in an HIV-positive pregnant Thai woman who was a former sex worker: Case study. , Archives of Psychiatric Nursing 21, 32-39.
- 22.Sawatphanit W, Ross R, Suwansujarid T. (2004) Development of self-esteem among HIV positive pregnant women in Thailand: Action research. , Journal of Science, Technology, and Humanities 2(2), 55-69.
- 23.Simbayi L, Kalichman S, Strebel A, Cloete A, Henda N.Internalized stigma, discrimination, and depression among men and women living with HIV/AIDS in Cape Town. , South Africa. Social Science & Medicine doi:, 10-1016.
- 24.Beck C. (2002) Postpartum depression: a metasynthesis. , Qualitative Health Research 12(4), 453-472.
- 25.Jirapaet V. (2001) Factors affecting maternal role attainment among low-income, Thai, HIV-positive mothers. doi: 10.1177/104365960101200104. , Journal of Transcultural Nursing
- 26.Ross R, Srisaeng P, Sawatphanit W, Draucker C.Worries among HIV-positive pregnant women in Thailand. Poster presentation at the 30th Midwest Nursing Research Society Conference , Milwaukee, WI .
- 27.E A Howell, Mora P, Leventhal H. (2006) Correlates of Early Postpartum Depressive Symptoms. , Maternal and Child Health Journal doi:, 10-1007.
- 28.Liabsuetrakul T, Vittayanont A, Pitanupong J. (2007) Clinical applications of anxiety, social support, stressors, and self-esteem measured during pregnancy and postpartum for screening postpartum depression in Thai women. doi: 10.1111/j.1447-0756.2007.00532.x. , Journal of Obstetrics and Gynaecology Research
- 29.Srisaeng P. (2003) Self-esteem,stressful life events,social support,and postpartum depression in adolescent mothers. in Thailand.Unpublished Doctoral dissertation,FrancesPayneBoltonSchoolof Nursing,CaseWesternReserveUniversity
- 30.Abramowitz S, Koenig L, Chandwani S, Orban L, Stein R. (2009) Characterizing social support: global and specific social support experiences of HIV-infected youth. doi: 10.1089/apc.2008.0194. AIDS Patient Care & STDs.
- 31.Prachakul W, Grant J, Keltner N. (2007) Relationships among functional social support, HIV-related stigma, social problem solving, and depressive symptoms in people living with HIV: a pilot study. , Journal of The Association of Nurses In AIDS 18(6), 67-76.
- 32.Bennetts A, Shaffer N, Manopaiboon C, Chaiyakul P, Siriwasin W. (1999) Determinants of depression and HIV-related worry among HIV-positive women who have recently given birth. , Bangkok, Thailand, Social Science & Medicine 49(6), 737-749.
- 33.Levine A, Aaron E, Criniti S. (2008) Screening for depression in pregnant women with HIV infection. , Journal of Reproductive Medicine 53(5), 352-356.
- 34.Wu Ying, Munoz D, Espiritu M, Zeladita B, Sanchez J et al. (2008) Burden of Depression Among Impoverished HIV-Positive Women in Peru. , Journal of Acquired Immune Deficiency Syndromes 48(4), 500-504.
- 35.Pakenham K I, Rinaldis M. (2001) The role of illness, resources, appraisal, and coping strategies in adjustment to HIV/AIDS: The direct and buffering effects. , Journal of Behavioral Medicine 24(3), 259-279.
- 36.Radloff L S. (1977) The CES-D Scale: A self-report depression scale for research in the general population. , Applied Psychological Measurement 1(3), 385-401.
- 37.Zimet G D, Dahlem N W, Zimet S G, Farley G K. (1988) The Multidimensional Scale of Perceived Social Support. , Journal of Personality Assessment 52(1), 30-41.
- 38.Zimet G D, Powell S S, Farley G K, Werkman S, K A Berkoff. (1990) Psychometric Characteristics of the Multidimensional Scale of Perceived Social Support. , Journal of Personality Assessment.55(3/4): 610-617.
- 39.Rosenberg M. (1989) Society and the adolescent self-image (rev.ed.).Middletown,CT,England:WesleyanUniversityPress.
- 40.B G Tabachnick, L S Fidell. (2007) Using multivariate statistics.(5th ed.).Boston,MA:Pearson/Allyn and Bacon.
- 41.Byrne B M. (2010) Structural equation modeling with AMOS: Basic concepts, applications, and programming,New York,NY:Lawrnece Erlbaum Publishing.
- 42.Hu L, Bentler P M. (1999) Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria Versus. Structural Equation Modeling. 6(1), 1.
- 43.Hartley C, Pretorius K, Mohamed A, Laughton B, Madhi S. (2010) Maternal postpartum depression and infant social withdrawal among human immunodeficiency virus (HIV) positive mother-infant dyads. , Psychology, Health and Medicine 15(3), 278-287.
- 44.Kapetanovic S, Christensen S, Karim R, Lin F, W J Mack. (2009) . Correlates of Perinatal Depression in HIV-Infected Women. doi: 10.1089/apc.2008.0125. AIDS Patient Care & STDs .
- 45.Chibanda D, Mangezi W, Tshimanga M, Woelk G, Rusakaniko S.. (November2010) Postnatal Depression by HIV Status Among Women in Zimbabwe. doi: 10.1089/jwh.2010.2012. Journal of Women’s Health .
- 46.Sullivan P S, Dworkin M S. (2003) and the Adult and Adolescent Spectrum of HIV Disease Investigators. Prevalence and correlates of fatigue among persons with HIV infection. , Journal of Pain and Symptom Management 25(4), 329-333.
- 47.Voss J, Portillo C J, Holzemer W L, Dodd M J. (2007) Symptom cluster of fatigue and depression in HIV/AIDS. , Journal of Prevention and Intervention in the Community.33(1-2),19-34
- 48.Barroso J, Preisser J S, Lesserman J, Gaynes B N, Golden R N. (2002) Predicting Fatigue and Depression in HIV-Positive Gay Men. , Psychomatics 43(4), 317-325.
- 49.Ferrando S, Evans S, Goggin K, Sewell M, Fishman B. (1998) Fatigue in HIV illness: relationship to depression, physical limitations, and disability. , Psychosomatic Medicine 60(6), 759-764.
- 50.Castrighini C, Gir E, Neves L, Reis R, Galvão M.Depression and self-esteem of patients positive for HIV/AIDS in an inland city of Brazil. , Retrovirology doi:, 10-1186.