
Abstract
We examined special roles of the Central Nervous System (CNS) in an attempt to resolve the puzzle that chronic diseases cannot be cured in medicine. By exploring a skill-learning model, we found that the CNS is able to remember certain information reflecting biochemical and cellular (B&C) processes in the body. From the skill-using ability, we found that the CNS is able to control basic B&C processes that drive and power the skill. From the ability to adjust forces and moving direction of body parts, we infer that the CNS is able to adjust B&C processes that control physical acts. From this controlling capability, we inferred that the CNS must also store certain information on the baseline B&C processes, is able to up-regulate or down-regulate the B&C processes, and make comparisons in performing its regulatory functions. We found that chronic diseases are the results of deviated baseline B&C processes, the CNS plays a role in maintaining deviated baseline B&C processes, and protects the body state of a fully developed disease. The three CNS roles can explain that cancer progresses with increasing malignancy, cancer quickly returns after a surgery, cancer cells repopulate after chemotherapy and radiotherapy, cancer patients develop drug resistance inevitably, immune cells rebound after suppression, etc. We further showed that long-term exercises generally can correct part of the departures in B&C processes and thus help to reverse chronic diseases. Finally, we propose strategies for resetting the CNS’ state memory as an essential condition for curing chronic diseases and cancer.
Author Contributions
Copyright © 2022 Jianqing Wu, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Chronic diseases cannot be cured by medicine, but we personally witnessed life miracles. Even based on isolated cases, we question the notion of incurable diseases. Neuronscience researches have resulted in a body of evidence of the roles of the CNS on chronic diseases and cancer. To find root reasons for failure to find predictable cures for incurable diseases, we examined the mind-and-body model which was once used in all medical systems in the world.
Fundamental hypothalamic systems control metabolism, circulation and the immune system 1. The functioning of these systems is strongly influenced by factors including sensory autonomic feedback and circulating hormones. The central and peripheral nervous systems play important roles in controlling liver cytochrome P450 (CYP) 2. The CNS is a mediating factor in the pathogenesis of diseases such as diabetes and hypertension. The hypothalamus at the intersection of the neuroendocrine and autonomic systems regulates glucose and blood pressure homeostasis 3. Acute and chronic psychological stress can increase the risk of heart attack by increasing circulating levels of platelet–leukocyte aggregates 4. Chronic stress is an emerging risk factor for heart diseases 5, 6. Stress increases the pro-inflammatory response in caretakers of Alzheimer’s patients 7.
A body of evidence has shown that the CNS regulates the immune system and inflammatory process 8. Stress makes humans susceptible to infection and negatively affects wound healing by disrupting the production of proinflammatory cytokines 9. Chronic stress plays a role in cancer proliferation and negatively affects immune system 10. Stress management can modify neuroendocrine dysregulation and immunologic functions and thus influence tumor development and progression 11. Stress-induced neuroendocrine activation induces a 30-fold increase in metastasis to distant tissues by β-adrenergic signaling, which increases the infiltration of M2 macrophages into the primary tumor 12.
About hundred billion neutrons in the brain are connected to all nerves with fibers in the tissues in every part of the body. Partially based on the relationships between the CNS and diseases, we suspected that the brain regulates the health state of the body, remembers information about the tissues as special state memory, and uses the stored information in up-regulating or down-regulating B&C processes for the body. Those functions would serve as a protective mechanism for maintaining the body’s stability but prevent chronic diseases from being reversed. If those CNS roles are confirmed, the failure to consider those roles would make all attempted cures futile or unpredictable.
Methods
Subtle and precise interactions between the CNS and the body cannot be studied in a controlled condition in current state of art. The capability of medical research art is limited to detecting neuronal signals from certain neurons such as genetically encoded voltage indicator (1997) and fluorescent labeled neutrons (2012). We believe that it would take centuries before the meanings of neuronal signals can be ever interpreted, and it would take even a longer time before the subtle differences in neuronal signals and their firing and traveling patterns can be accurately linked to chronic diseases.
The three CNS’ roles that we are now trying to prove here would directly affect medical landscape. If the CNS actively records disease information and uses recorded information to maintain disease condition, a cure will not succeed unless effective measures are directed to the CNS. The three roles will affect medical research model, treatment model, personal health management, and achievement of longest personal lives, etc.
One of the authors started thinking potential CNS roles two decade ago. Despite rapid developments in neuron-science, no direct evidence is still unavailable. However, evidence discovered in the last two decades allows us to prove the three CNS roles indirectly. We will prove them by relying on common knowledge, personal experiences, and accepted knowledge.
Evidence that the CNS regulates B&C processes are systematically reviewed to understand how the CNS regulates basic metabolism, the immune system, hormonal functions, etc.
Primary evidence is extracted from a skill leaning model. Every person knows how to learn a skill of performing a physical act such as a triple loop in ice-stating. One advantage of using this approach is everyone’s experience and thus every person can appreciate implied and derived subtle facts. Such a learning model vividly reveals how the CNS and the body interact in every increment of time. Human beings as well as some animals have three abilities: skill learning ability, skill refining ability, and skill reusing ability. By analyzing detailed activities of the CNS and the body for the three activities, we extract evidence in support of the three CNS roles.
We then apply the three CNS roles to solve several puzzles, conflicts and controversies in cancer researches to test whether they reasonably reflect the working in the human body. While our test is limited to cancer, the findings can be used to resolve puzzles in other chronic diseases such as obesity, high blood pressure, heart diseases, metabolic syndrome, etc.
Results
To show how the brain remembers information concerning B&C processes, we will consider how a person learns the skills of performing a physical act.
Evidence of the CNS Memory of B&C Processes
The skills of performing physical acts can be remembered. After a person has learned swimming or riding a bicycle, such skills are “remembered” as explicit memory. The person can still swim or ride a bicycle many years after disuse of the skills. However, neither “skills” nor “acts” can be stored in the brain. What could be stored are information that would be used in generating neuronal signal firing patterns that control a series of physical acts for the skills.
When a person performs a physical act such as making a triple-loop in ice-skating, the act is driven by a series of neuronal signals which modulate B&C processes. Such a physical act was believed to be driven by motor functions involving both the primary motor cortex and secondary motor cortices.
Motor functions and sensory functions cannot take place without the support of underlying B&C processes. Since B&C processes must run in the baseline levels, every physical act can be traced to changes in B&C processes in different parts of the body. Each physical act is driven by CNS signals or environment stimuli (as in an involuntary case). In both situations, the CNS sends distinctive neuronal signals (for convenience, we use neuronal to means neural as well) to relevant parts of the body. Such signals cause different muscles to contract and cause different body parts to collaborate in right forces, directions and timings. In addition, the CNS also regulates heart beat rate, nerve signaling activities, body temperature, organ operating capacities, etc. In performing the act, the CNS must also get from the body feedback neuronal signals to be used as the basis for adjustments of subsequent signals. For a physical act, the brain generates a distinctive neuronal signal pattern -- different neuronal signal activities in different parts of brain in different time. Detailed real-time neuronal patterns cannot be acquired due to overwhelming difficulties of the subject and limitations of current technologies, but evidence of changed brain neuronal signal patterns in a controlled state can be acquired by using NMI technologies 13.
When a person performs a triple loop jump, the first driving force is the desire or thought. It sounds absurd, but if the person does not want to do, there would be no tripe loop. We do not want to explore this because it is beyond our ability and scope of this study. After whatever happens in the brain, the CNS sends neuronal signals to cause the legs to generate a large amount of force. When the body is spinning in the air, the CNS’s sends signals to different parts and receives feedback signals from different parts in an attempt to maintain body balance in the air, to cause the body to do all necessary acts to facilitate the body’s rotation in the air. At the time of landing, the body prepares the feet for absorbing force. The jump involves the firing of neuronal signals which are expected to influence the following functions:
Alter B&C processes for different parts of the body in a time-dependent course. For example, at the moment of jumping up, a great force is generated in the leg muscles responsible for the jumping;
Make different parts of the body to cooperate when the body is spinning in the air. The body tries to maintain proper shape and position in every time interval;
Improve the body's ability to detect spatial position. The body must jump to a right height, and rotate in a suitable speed so that three loops will be finished at the moment that the body touches the ground;
Force the body to make adaptive changes in the structures and functions of the body to support the skill. A long time training program will cause the body to develop strong bones, strong muscles, and strong joints. We should find that such neuronal signals of the CNS can cause the body to slowly alter body structures; and
A large number of other changes occur to support the skill. In each attempt, the CNS and the body must exchange neuronal and neural signals.
We show that each of the component act is backed up by B&C processes as shown in table 1 below.
This table is not intended to include all details. Involved B&C processes include metabolic processes for proteins, glucose, fats, etc. They could include carbohydrate metabolism (glycolysis, Krebs cycle, pentose phosphate pathway, etc.), cellular respiration, amino acid metabolism, nucleotide and protein metabolism, lipid metabolism, cell signaling, vitamin and co-factor metabolism, etc. It is assumed that all other metabolic processes are altered in response to every increment of the tripe loop.
Table 1. Physical Activities and Neuronal Signals for Performing A Triple Loop.| Physical Act | Directly Involved B&C Processes | Controlling Signals | Baseline B&C Processes | References/Comments |
| Jump force. | Sliding filaments in the leg muscles. | Impulse frequency and number of motor units. | Controlled by neuronal signals (action potential and motor units). | Implied. |
| Body orientation. | Sliding filaments in different parts of muscles. | Same as above. | Same as above. | Common sense. |
| Boy parts collaboration. | Sliding filaments in collaborative parts. | Same as above. | Same as above. | Common sense. |
| Regulation of metabolism (ATP). | Increase energy production for the whole body by blood circulation system. | Alter the vascular system and involved muscles. | Raise energy production over baseline values in involved muscles. | All metabolic processes involving glucose, protein, fats, etc. |
| Actions caused by ASN. | Make a fight-and-flight like adjustment for the body. | CNS signals, ASN actions, and hormonal actions. | Up- and down- regulation, depending on parts or organs. | A large number of different changes are well known. |
| Inhibit other CNS activities. | The requirement of focus will lead to highly inhibited state. | Inhibit neuron activities that are not required for the triple loop. | Down-regulation or push below baseline values. | Common sense, personal experiences, and ancient teachings. |
| Waste removal. | The normal processes. | Implied. | ||
| Physical properties adjustments. | Temperature, pH, mechanical properties, etc. | Changes over baseline values. | Perceivable by anyone. | |
| Adaptive changes in body structures. | Affect capillary density, bone strength, and nerve action efficiency, etc. | Changes over baseline body structures. | It works by long-term effects. |
The actor is able to make incremental adjustments: when an early part of the loop is poorly executed, he can make compensatory measure to make successful landing. This is observed in any of those failed performance. This implies that the CNS must get feedback in every incremental time and can change B&C processes attributes in support of the skill. Since the person can reuse the skill, the CNS must be able to use stored information which can control B&C processes that drive the skill. Both skill-recalling capability and skill-refining capability imply that the CNS can remember certain information which is essential for performing a triple loop.
Evidence of the CNS Comparative Mechanism For Controlling B&C Processes
The skill-refining model implies that the CNS can cause the body to adjust the amount of force and force-applying directions by changing B&C processes. In executing a triple loop, the person can learn how to achieve a suitable jump height by keeping jumping while trying to control force amount and force-applying direction. The exact mechanism for making adjustments is not necessary to make this factual finding. If a prior jump fails to reach a required height, the person can try another jump by applying an increased amount of force. This implies that the CNS not only remembers the amount of force and force direction used in the prior jump, but also knows how to change them in a quantitative way. This ability is extraordinary: after a person is presented with three persons’ photos, the person can identify them. This ability implies that the CNS is able to make comparisons, which will be referred as the comparative mechanism. The CNS must use its own comparative mechanism in making a comparison.
The comparative mechanism is actually frequently used in humans in applying force. Adjustment of amount of force and direction of force for a physical act can be realized only adjusting B&C processes against baseline values in different parts of the body. Human body does not have things like electrical motors, engines, or force-generating mechanical devices. Since each physical act is driven and powered by B&C processes, the body must have a way to adjust B&C levels. The feedback mechanism also implies that the CNS must “know” the baseline values of B&C processes or prior B&C processes. The baseline values are the values of B&C processes that do not cause the body to generate force under given temperature, pH, mechanical activities, etc.
If a person wants to apply about 1 lb more force in a certain direction, the CNS must have an ability to adjust muscle groups, motor unit pool and motor unit (the number of muscle fibers innervated by the neuron), impulse frequencies, etc. in a reasonable accuracy so that about 1 lb more force will be generated. Regardless of the complexity, the adjustment must be originated from the intention or desire, the final results are reflected in the force and force direction. The feasibility of this adjustment depends on the CNS ability to recall muscle groups, motor pool, motor units, control impulse frequencies, etc. in prior jumps. This ability is like a person’s ability to recall visual impression of an object that the person has seen many days before. If the CNS could not recall any prior force-related information, the person may apply far too much force or too little force. Without this accurate comparison mechanism, human acts would be erratic and unpredictable, and all humans can do are accidents and controllable destruction of properties.
Human ability to improve accuracy of physical acts is reflected in how a person can improve accuracy of throwing a dart on a target. The first a few throwing attempts by a person may miss the target by large margins. However, if the person keeps practicing, he normally can improve throwing accuracy slowly and consistently. Some persons can achieve very high accuracy in hitting the target. Such progressive improvements imply that the CNS has a comparative mechanism to adjust force amount and force direction in very high reliability in most normal persons. We infer that improvements can be achieved ultimately by adjusting B&C processes against baseline or prior B&C processes.
Quantitative adjustments of force and force direction can be explained by the sliding filament theory 14. The force generating unit of muscles comprises actin and myosin chains, which can slide past one another. Ignoring details, energy for the release and movement of the myosin head along the actin filament comes from ATP, which is produced in metabolic processes. The force generated is proportional to motor pool size, motor units, frequencies of the impulse signals, etc. To increase force, the CNS may use more motor units, raise frequencies of the impulse signals, or do do both. The relationship between the frequency of the impulse signals and the contributory force of a single motor unit must be predictable so that the CNS can adjust the amount of force in reasonable accuracy. While the number of motor units and the frequencies of the impulse signals directly affect force, muscle contraction force is ultimately limited by energy availability. Each of those changes is driven by related B&C processes under the control of the CNS signals.
Baseline B&C processes in the human body are like operational baselines in machines such as car idle engine speed, a scale’s tare reading, spectroscopic baseline signals, etc. Baseline-like things must exist in the human body except that they are ultimately defined by attributes of B&C processes. Their existence does not necessarily depend on the correctness of the sliding filament theory or other theories used to explain the force-controlling mechanism. If the sliding filament theory is wrong or only partially correct, there must be an alternative force generating mechanism.
In performing a triple loop jump, actual B&C processes must be altered according to required force and force direction in different parts of the body. In preparing for the jump, the body takes a lower position which can help to generate more force. In making the jump, the body generates great force suddenly. In both the preparation moment and jumping moment, different muscles run B&C processes at suitable levels. The CNS signals can cause the body to make qualitative adjustments of states. In performing each of the incremental steps, the CNS selects different muscle groups, uses different motor units, and apply different impulse frequencies to achieve right amount of force in right force directions. In each case, the CNS must know and use the baseline B&C values.
Neuronal signals that drive a physical act, if viewed on a time course, may comprise component neuronal signals, transmitting from different parts of the brain through different channels to nerve fibers or motor units in different parts of the body in different time increments. Muscle contraction is not the only activity for performing the act. The neuronal signals must include other components for up- and down-regulating various B&C processes in different parts or organs. In addition, the physical act may be accompanied by corresponding changes which may be triggered, for example, by the autonomic nervous system.
A comparative mechanism is also implicated in perceiving sensory properties such as temperature, structures, smells, vibrations, textures, colors, etc. It is also used in perceiving complex things such as a room’s comfortable levels, element patterns in an image, moving trajectories of multiple objects, light flash patterns (as in Christmas trees), etc. The information to be compared must involve the use of B&C processes.
Evidence of the CNS’ Regulation of Body State
When the person reuses the skill of performing a triple loop, the person causes the CNS to replay the neuronal signal firing pattern for the skill. The neuronal signals cause the body to up- and down-regulate B&C processes for different parts of the body in a time-dependent manner. The neuronal signals reflect or are influenced by certain information that is once stored as state memory. This memory is similar to implicit memory in psychology, but our focus is not on information that is studied in psychology. What we are interested is the portion of information that is directly responsible for controlling B&C processes which affect body physical act, organ functions, physical properties, body structures, etc. For this reason, we refer it as state memory despite its similarity to implicit memory. State memory is stored information, which, upon being called to run in the brain, can generate the same neuronal signals pattern that drives the B&C processes which drive the skill.
In using the skill, the up- and down-regulation of B&C processes cannot be realized without “using” correspondent baseline B&C values. For example, when the body is in a preparation stage, the legs exert little force. To make the body to jump to certain height in a right direction, the CNS signals must cause the body to increase force by a right amount and use different muscles. We infer that the CNS has a mechanism to determine how to change the B&C processes for each increment of time in performing the act. If we focus at the B&C processes, all the CNS does is to change relative speeds of various involved B&C processes in different parts in different times.
When a person performs different physical acts, the CNS sends different neuronal signal patterns. While swimming, riding a bicycle, performing a triple loop, and doing anything look different, they are driven by the same B&C processes. The only differences are the relative speeds of different B&C processes in different parts of the body in different times.
Implied by the subtle facts, what is actually remembered is information carried in the neuronal signal patterns, which, after transmitting to multiple target tissues, are able to alter B&C processes that drive the physical acts. Stored information is retrieved from the brain to be used to regenerate the same neuronal signal patterns that drive the same acts. In order to conduct up- or down-regulation of the B&C processes, the CNS must use respective baseline B&C values in the relevant part of the body in every increment of time.
At the level of muscle contraction, adjustments to force and contraction velocity are in part based on muscle tone. Muscle tone is the state that muscles are in partial contraction, which is important for generating reflexes, maintaining posture and balance, and controlling other function of organs such as the heart. Muscle tone is controlled by the sensory muscle spindle, which measures muscle stretch. At this level, the CNS must be able to track muscle tone as well as the incremental state of muscle contraction. Each of incremental contraction is ultimately driven by relevant B&C processes. What the CNS can alter are the speeds of relevant B&C processes in different parts of muscles, tissues, and organs in different time increments. Comparisons are used in the learning processes and the refining processes.
The state memory is not limited to learning skills. It is also reflected in forming habits, personalities, likeness, face durable looks, etc. The CNS must maintain the state of the person. It implies that if a person has acquired a chronic disease, the state will be accepted by the CNS and information about the diseased state is recorded in the brain, it is hard to change. This is why it is hard to change habits, tastes, and likeness. That is why it is hard to reverse chronic diseases. We attribute chronic diseases state, tendency of disease relapse, and increased cancer malignancy to this kind of state memory.
The CNS can cause body structures to make adaptive structural changes. Marathon runners can develop strong legs; martial artists may develop unique strong parts, depending on the arts they practice; bicycle riders develop leg features suitable for doing large circular motions; and people who carry loads regularly on shoulders can build stronger shoulders. Exercise may increase muscle fiber number in each involved motor unit and help the body to develop large motor pools. The CNS neuronal signals can influence body structures by long-term effects.
Neuronal signals must be the kind that can influence B&C processes that are fully supported in genes. Available B&C processes that the CNS can regulate must exist or could exist in the body. However, neuronal signals may directly or indirectly affect gene expression signatures which thus affect the speeds of some B&C processes.
Chronic Diseases are Reflection of Deviated B&C Processes
We now extend CNS state memory, CNS regulatory function with comparative mechanisms established on the skill model to chronic diseases. While the skills of performing a physical act appears to be very different from chronic diseases, they must share common or basic B&C processes. We will show chronic diseases are results of deviated B&C processes.
Chronic diseases are developed in time windows from years to decades. One definition best reflecting the development time is provided in Booth et. al.15. The long development time implies that the body slowly loses its functional capacity for maintaining life. Functional capacity ultimately comprises a large number of B&C processes. What is much detrimental are lost imbalances. Functional imbalances include biochemical process imbalance such as more calories being stored than used; structural imbalance may be outgrown tissues and bones in permitted spaces or lost tissues; material demand imbalance, for example, occurs when oxygen provided is insufficient for sustaining threshold metabolism; and physical property imbalances include deviated body temperature, deviated blood fluid pH, and altered mechanical properties (e.g., increased blood viscosity). A long development time of chronic disease implies that observed structural changes are very small in given times.
We will show exercises, chronic diseases, and cancer can constantly interact with each other through their shared baseline B&C processes. Diseases cannot create a new B&C process that does not exist in the genes of the mankind. “No cancer exhibits any trait which cannot be found in some normal tissue as the expression of normal genomic activity.” 16. The most the CNS could do is to alter gene expression signatures which affect some aspects of relevant B&C processes. Most, if not all, chronic diseases are manifested finally as structural changes. Structural changes in body parts or organs can be caused only by altered, abnormal or imbalanced B&C processes. The long development time implies that small deviations in the B&C processes can cause chronic diseases by their long-term effects.
Chronic disease development, cancer development and long-term exercises like performing a triple loop all influence shared baseline B&C processes. Their common effects are shown in table 2 below.
Table 2. B&C Processes For a Triple Loop-induced State, Chronic Diseases and Cancer.| Events(Skill or Diseases) | Basic B&C processes | Changes in B&C Caused by Event | Most Important Changes Caused by Event | Duration of Changed B&C Processes |
| Triple Loop. | All known B&C processes. | Changes caused by event appear as deviations from baseline values. | Energy metabolism, nerve functions, and vascular system. | Temporary or as peaks, but subside slowly. |
| Chronic Disease. | All known B&C processes. | Changes are merged into the baseline values as new abnormal baselines. | All potential epigenetic changes, depending on diseases. | Permanent (as baseline B&C processes values). |
| Cancer. | All known B&C processes. | Changes are merged into the baseline as new abnormal baselines. | Gene expression signatures; agiogenesis; neurogenesis, growth levels, apoptosis, etc. | Permanent (as baseline B&C processes values). |
Since a chronic disease exists on a 24-hour basis, deviations of baseline B&C processes are merged into baseline values and appear as new abnormal values. If a person's blood vessels are plagued slowly, blood pressure at rest condition will go up slowly but further higher blood pressure appears when the person does exercises. Similarly, if a person's liver, kidney, or lung functions are diminished, the state would exist on a 24-hour basis.
Figure 1 shows how exercise, disease, and cancer affect B&C processes and permanently change state. Since B&C processes cannot be characterized easily, we will use certain health properties that reflect B&C processes. The properties shown in Figure 1 include blood pressure, systemic inflammation, tissue temperature, absolute metabolic level, toxic removal rate, mechanical properties, CNS emotional responses, etc. Each of those health properties reflects some relevant B&C processes. As indicated by the black arrows, a chronic disease alters baseline B&C processes slowly, causes some properties such as blood pressure, systemic inflammation level, CNS emotional responses to shift upwardly, but cause other properties such as tissue temperature, mechanical activity level, etc. to shift downwardly. The red lines were where the affected B&C would be. Figure 1 shows only some health properties that are most important for chronic diseases, but any of a large number of other health properties might be involved. Moreover, an identical health property may behavior differently in different persons, depending on tissues or organs.
Figure 1.Changes in B&C processes caused by diseases, cancer and exercise are relative to shared baseline B&C values.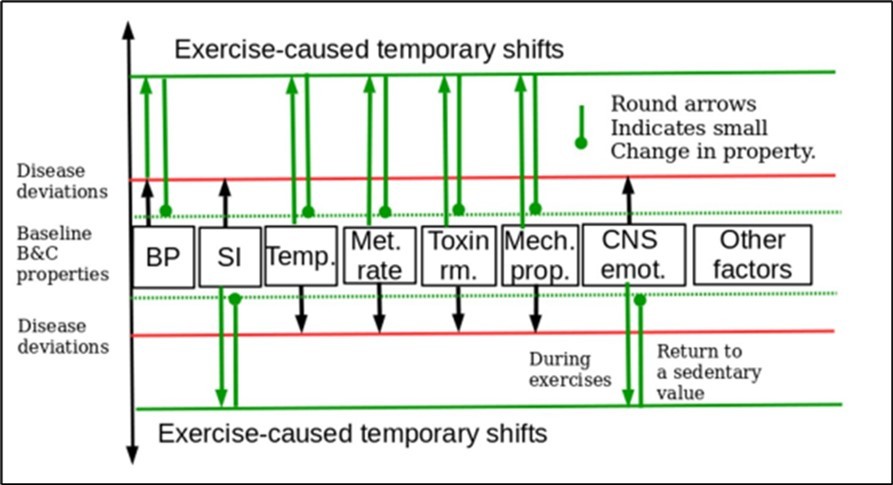
Figure 1 shows that exercises have both instantaneous effects and long-term effects. Exercises raise blood pressure temporally, but removed fats allow blood pressure to go down slowly. Long-term exercises slowly reduce systemic inflammation level. Exercises can raise body temperature slightly within the normal temperature ranges, increase the tissue’s mechanical vibrations, and improve the body ability to remove toxins. Exercises temporarily inhibit emotional hormonal activities. Exercises are expected to cause the Autonomic Nervous System (ANS) to take a number of well known coherent actions. As shown by two dashed green lines in Figure 1, exercises can slowly correct deviations in baseline B&C processes by long-term effects.
We have shown that human beings must maintain the stability of baseline B&C processes. Changes caused by physical acts and deviations caused by diseases cannot have any meaning if they are not referenced to respective baseline values. The execution of a physical act depends on the CNS ability to know baseline B&C processes. Similarly, effects of emotional factor depends on the CNS ability to know baseline B&C processes. The ability to maintain baseline B&C processes is essential for maintaining the stability of personal looks, size, health condition, physical strength, personalities, etc.
Based on the above derived facts, we found that the CNS stores as a special state memory, information on deviated B&C processes, and the CNS attempts to maintain deviated B&C processes. We therefore conclude that the CNS state memory is responsible for maintaining the state of an existing disease.
Additional Evidence of the CNS’ Memory
State memory of the CNS is reflected in how the body keeps same looks, same habits, same homeostatic properties, same likeness in tastes and smells, same circadian cycles, same personalities, etc. None of those things can be directly stored in the brain as memory. What can be stored is information that can control B&C processes for controlling those properties. Each of those properties is related to B&C processes: looks reflect facial structure which is a result of B&C processes; habits are physical acts that are driven by B&C processes controlled by CNS neuronal signals; likeness in tastes and smells are controlled by B&C processes in sensory functions; circadian cycles are controlled by certain B&C processes; and personality is a reflection of thinking processes that are driven by B&C processes.
State properties are maintained by using information that controls the characteristics of B&C processes. Such information, upon running, generate neuronal signals that control the relative speeds of B&C processes and interactions of different B&C processes in different parts of the body in different times. If any B&C process that affects any healthy property is changed, related health property will change accordingly. The state memory of the CNS is an essential component for maintaining the stability of the body’s structures and functions.
Another piece of evidence of state information is the fact that a person can still feel pain of a diseased limb even after the limb has been amputated. This fact demonstrates that the pain is a replay of stored state information reflecting the amputated limb but not just a result of a stimulation of diseased limb.
Figure 1 indicates that exercises can correct deviated B&C processes in a way no medicine can.
The CNS Role from Cancer Initiation To Spreading
Cancer becomes a puzzle for more than a century. Although cancer progression may occur through clonal evolution 17, potentially the full malignant potential of a cancer is present at the time of cancer cell transformation 18. Cancer point-mutation rates are comparable to normal cells, progression from a large adenoma to cancer require about 17 years, and generally the same mutations are present in primary tumors and their metastases 19, 20, 21. Increasing malignancy in cancers cannot be explained by clonal selection of mutations in most cases. Cancer can occur without mutations or mutations may be product of cancer. Revolving around this progression puzzle are a large number of phenomena such as cancer cell repopulation, increased cancer proliferation speeds, shorten time for cancer returning, and increased drug resistance, etc., all of which are responsible for cancer's hazard. Cancer develops from struggles to triumphs. We show that the CNS is a dual-edged sword. It first does whatever it could to prevent or stop cancer proliferation, and, in a later phrase, does whatever it could to promote cancer growth.
Cancer's Early Struggles for Survival
Assuming that a set of mutated cells C1, C2,…., Cj formed in a tissue or an organ in different times from age one to age 40 (See Figure 2), each of the mutated cells has a potential to become a cancer but none can gain momentum of proliferation. Some cancer cells become extinct; but others stay in dormancy for long times. If there is not cancer driving mutation, there might be cell alterations that initiate cancer.
Figure 2.Clonal expansion in a primary site, with help of the CNS, promotes cancer growth and increases cancer malignancy.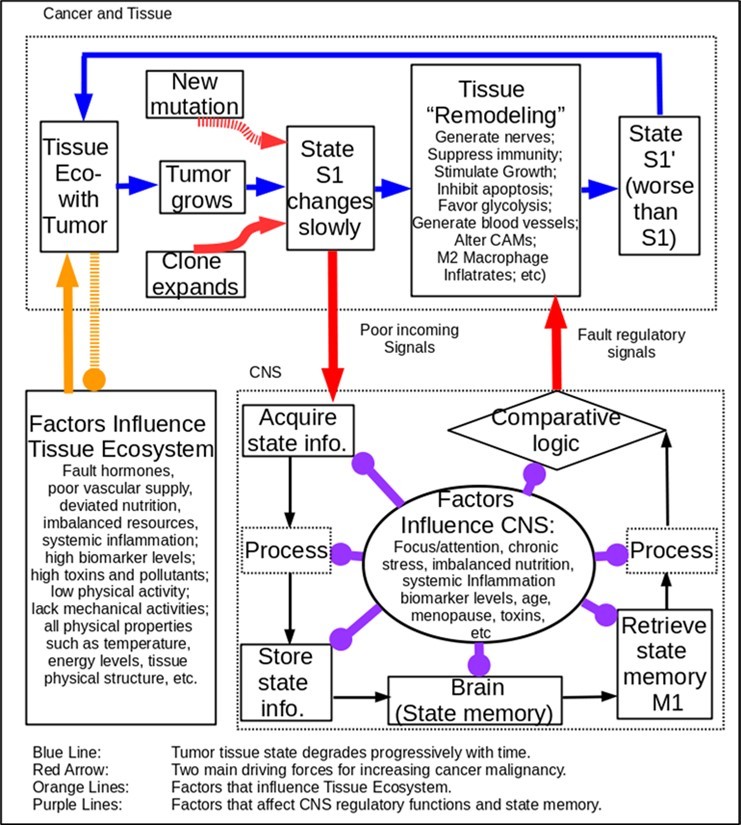
In the early stage, the cancer does not have dominant influences in the tissue, and the CNS regulates the tissue with an attempt to inhibit clonal expansion. A cancer initiation requirement is a faulty tissue micro-ecosystem, which reflects a big mismatch between the living environment of human beings and that human genes are adapted to 22. As shown in Figure 2, the tissue ecosystem further degrades as a result of strikes of chronic stress, systemic inflammation, infection, trauma, foreign objects, etc. Existing mutations and degraded tissue ecosystem slowly favor cancer initiation and proliferation.
The information on the issue’s state is carried in the signals transmitting to the CNS and saved there in some way. The state memory is stored in the CNS like a re-writable media of computer; and stored information in the CNS is slowly altered with increasing tumor size and degrading tissue ecosystem. The CNS’s ability to contain cancer becomes weaker and weaker with aging. Moreover, emotional distress, chronic stress, chronic inflammation, etc. slowly weaken the CNS's ability to discriminate against survived cancer cells. Other factors affecting CNS control include hormonal disorders, menopause, aging, imbalanced nutrition, faulty lifestyles, etc. Those factors help cancer cells to gain progression momentum. A cancer cell with mutations accumulated at young ages may increase its growth speed at a late age.
After the cancer has reached a sufficiently large number of clones, destroying the tumor would be too dangerous for the host body. The CNS will change its role from rejecting and inhibiting cancer cells to accepting and protecting cancer cells. This is done by using the comparative mechanism shown inside the CNS block in Figure 2. Only the CNS has an inhere ability to make such a determination. By altering neuronal signals (e.g., the red arrow), the CNS instructs the immune system to protect the tumor, and attempts to remodel the tumor tissue.
Development of Nerve Networks in Tumor
Due to chaotic inner structures, or diminished CNS regulatory capacity, the cancer’s B&C processes are disrupted. The inner tissue of the tumor lacks normal nerve networks 23. It is predicted that what the CNS detects is an unhealed wound with growth deficiency. To fix the problem, the CNS must find a way to communicate with the tumor before it can instruct the tissue to remodel itself. The CNS’ control of cancer depends on nerve fibers inside the tumor even when the cancer proliferates. Cancer and the nervous system can communicate 24, 25, 26. When cancer spreads, immune functions, inflammation, organic micro-environments and bone marrow are involved 27, 28, 29, 30, 31, 32, 33.
Due to chaotic structural organization inside the tumor, communication between the tumor and the CNS is expected to become worse and worse with the tumor growing. The CNS thus must attempt to regulate tumor inner tissue. One required condition is that the CNS needs nerve supports inside tumors. The connections between the CNS and cancer through synapse, non-synapse or humoral modulation make it possible to establish reciprocal interactions and communications between cancers and the CNS. Neuro-neoplastic synapses exist between nerve fibers and tumor cells 34, 35, and that neurogenesis, like angiogenesis, is also a trait of cancer cells 34, 35, 36, 37, 38. In primary and pre-metastatic sites, cancer cells can actively establish connections with nerve fibers and receive signals from the CNS. Even bone marrow can be innervated by the nervous system, including the ANS and noradrenergic sympathetic nerve fibers 39, 40, 41, 42, 43.
The CNS can communicate with the immune system by bidirectional neural-immune interactions. Their interactions mainly take place through the neuronal and immune signal molecules including hormones, neurotransmitters, neuropeptides, cytokines or their receptors, all of which have been demonstrated to contribute to the process of metastasis 44, 45, 46.
The CNS Cripples Anti-Tumor Immunity
Cancers have aptly been described as “wounds that do not heal” to indicate the similarities of their tissue environments 47, 48. Macrophages can exist in a spectrum of species from M1 type to M2 type 49. They play different roles in wound healing. M1-like types have strongest anti-cancer immunity. M2 macrophages, which are present later in the healing process, antagonize the inflammatory response and allow initiation of healing. The M2-like macrophages produce anti-inflammatory cytokines, suppress anti-tumor immunity, and promote angiogenesis and matrix remodelling, which favors tumor progression and metastasis 50, 51.
By relying on the shaky nerve network, the CNS regulates anti-tumor immunity by controlling Tumor Associated Macrophages (TAMs) (See “Tissue Remodeling” in Figure 2). Possible changes include those that are summarized in Noy and Pollard 52, as follows:
1. TAMs express effector molecules including cell surface receptors, cytokines, chemokines and enzymes and thus inhibit immune responses by interaction of TAMs receptors ligands with their counterpart death/inhibitory receptors expressed by the target immune effector cells.
2. TAMs also express the ligand receptors for PD-1 and CTLA-4 that upon activation suppress cytotoxic functions of T-cell, NKT cells and NK cells.
3. TAMs also express the ligand for the death receptors FAS and TRAIL that triggers in target cells caspase dependent cell death (apoptosis).
4. TAMs also express the non-classical HLA-G that inhibits T cell function through interaction with the co-stimulatory signal of T cells ILT2, and HLA-E that inhibit NK cells through CD94 (also known as NKG2).
5. TAMs secrete the cytokines IL-10 and TGFβ that inhibit T cells effector functions and induce regulatory functions, and chemokines CCL5, CCL20, CCL22 that recruit nTreg cells.
6. TAMs secrete Arginase I that inhibits TCR ζ chain re-expression in activated T cells by the depletion of L-arginine.
By all of those actions, the anti-tumor immune responses are inhibited.
The CNS Orchestrates Tissue Remodeling
To cure the “unhealed wound” as part of the tissue remodeling effort, the CNS takes concerted and coherent regulatory actions to promote healing. The CNS cannot send neuronal signals both to protect cancer cells on one hand, and destroy them on the other hand. The regulatory coherency of the CNS is a nature acquired in evolution. The CNS not just cripples the immune system, but also causes macrophages to switch from M1-like types to M2-like types, and uses them as arms to remodel tissues and resolve inflammation.
The inner region of the tumor is expected to have inferior nerve fiber networks than those in normal tissues. What the CNS detects is a tissue having diminished metabolic levels and diminished growth potential. To the CNS, cancer is an “unhealed wound.” Thus, what the CNS naturally does is to remodel the tissue: it causes the cancer-residing tissue to raise growth signals to encourage inner cells to grow, make cancer tissue insensitive to anti-growth signals, reduce cancer cell death speeds by disabling cell apoptosis, build more blood vessels to improve blood circulation, and lift cell replication number limit to allow more or unlimited cell divisions, etc. All of those actions will promote cancer growth. Those are well known B&C processes in cancer biology 53.
Other cellular processes regulated by the CNS range from general cell metabolism and to cell specific processes, such as differentiation, morphology, motility, secretion, neurotransmission, and gene transcription. As a part of remodeling effort, the CNS instructs the tissue to repress transcription of cell-to-cell adhesive molecules (CAMs), proteolyze the extracellular cadherin domain, switch expression of N-CAM from a highly adhesive isoform to poorly adhesive form, and changes expression of integrin subtypes.
The remodeling effort will reach other parts of the body. The CNS may recognize tissues by secreted chemicals and produced proteases. The CNS may use cancer secreted chemicals including cancer biomarkers as identification of cancer cells. If such chemicals are found in a secondary tissue, the CNS treats the cancer cells as remodeling subjects. The CNS protects any tissue that is permeated by such biomarkers. The host person eventually loses immunity against the cancer in all parts of the body, and the cancer can grow with little restrictions.
In the primary tumor, an excessive number of cancer cells crowd in a restricted space with unfavorable nutritional competition. Thus, it is more favorable to move cancer cells to new locations. The most widely observed changes are impaired cell-to-cell adhesive molecules and the docking of active proteases on the cell surface which can facilitate invasion by cancer cells into nearby tissues. The docking of active proteases on the cell surface can facilitate invasion by cancer cells into nearby stroma, across blood vessel walls, and through normal epithelial cell layers.
The cancer changes its state from S1 to S1’ in Figure 2. The cycle shown in blue arrows can keep going on a daily basis. Progressive changes in the CNS's state information is written as the CNS state memory. The state memory changes from the type with an effect of rejecting cancer cells to the type having an effect of protecting cancer cells. What the CNS achieves is increasing cancer growth speed, helping cancer cells survive, and promoting cancer metastasis. The remodeling efforts result in maximum cancer malignancy.
The CNS Learns “Bad” and Forgets “Good”
The CNS has many nerve axes. One example is gut brain axis. The gut is bidirectionally connected with the nervous system through the so-called “gut-brain axis” (GBA), which includes the central nervous system (CNS), the autonomic nervous system (ANS), the enteric nervous system (ENS), the hypothalamic pituitary adrenal (HPA) axis and the entero-endocrine system (EES). Hormones and neuro-hormones secreted at each of these listed GBA levels may modulate the gastro-intestinal digestive and metabolic activities, and vice-versa 54. One can infer that neuronal signals traveling in the axis affect tissue ecosystem where a tumor may reside. After the CNS uses and remember cancer-promoting signals, it forgets how to use those axes correctly.
The CNS Uses Learned Skills to Promote Cancer Growth
The CNS regulatory capabilities were acquired in evolution, and thus are built in human genes. The CNS starts using regulatory capabilities since the birth. The CNS learns regulatory capabilities whenever there is a first need. For an adult person, most of regulatory capacities might have been used. After the CNS regulatory capabilities are slowly altered as an attempt to adapt to tumor growth, the CNS masters the new capabilities like an acquired skill, and can use them onto other tissues. The changes caused by CNS regulatory capacities may include altering gene expression signatures.
The diversity of regulatory capacities determines how cancer can differ and change, how different cancers behave in the body, and how cancers evade drug actions, how cancer cells repopulate after they are surgically removed, etc. The cancer's apparent ability to evade cancer treatments actually reflects the intelligence of the human brain. That is why cancer is hard to defeat.
We believe that the CNS's adaptive changes play even a bigger role than clonal selection and tissue ecosystem alternations. We could view each cancer as a masterpiece of the CNS. It is the best way to explain the Bernards' cancer progression puzzle. Any attempt to fix one of a large number of immune system properties or one single health property will invite counteracting responsive actions of the CNS. That is why single or a few drugs cannot cure cancer, and nor chronic diseases.
The CNS Promotes Future Cancer Using Acquired Skills
We will show how the primary tumor influences cancer metastasis through acquired “skills.” As shown in Figure 3, the CNS can use its acquired skills to make another masterpiece cancer at a new site or distant tissues.
Figure 3.The CNS promotes metastasis and future cancer by sharing acquired “skills”.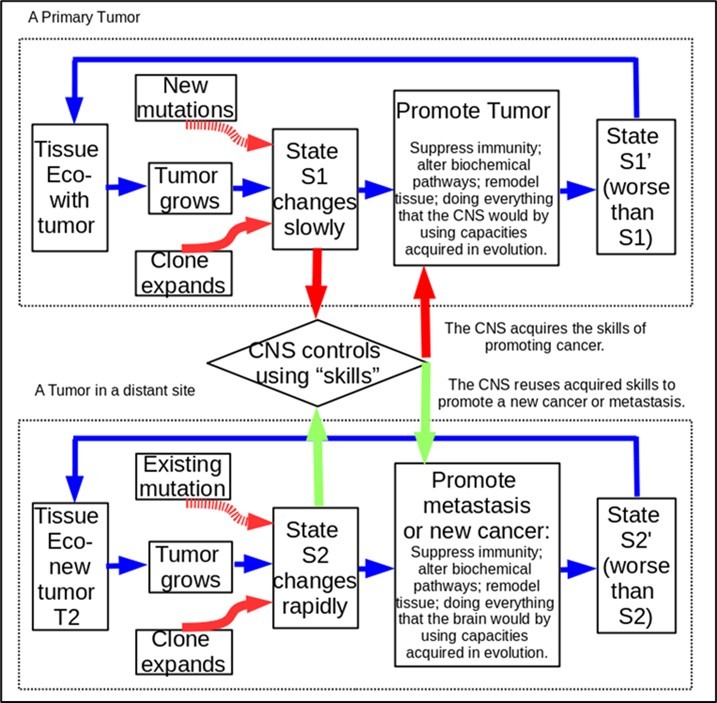
As long as the CNS has learned to protect and promote the primary cancer, it can teach the body to promote a new cancer’s growth at faster speeds. This is like reusing a skill that a person has acquired. Compared with normal neuronal signals, cancer-promoting neuronal signals reflect a large number of alterations which have an effect to up- and down-regulate B&C processes in different parts of the body. In addition, the CNS may alterate gene expression signatures for oncogenes and tumor-suppressing genes, and expressions of genes affecting neurogenesis, agiogenesis, cancer cell growth, etc. Even after the primary tumor has been removed, the cancer-promoting neuronal signals remain in the state memory.
The CNS uses the acquired “skills” to promote cancer growth. For example, raised inflammation levels for the body will cause the CNS to attenuate immune response including switching macrophages from M1-like to M2-like types. Figure 3 shows that the CNS can use the same skills from the primary tumor to a metastasis site. The CNS orchestrates bone marrows to produce more monocytes for generating M2-like macrophages in an attempt to repair the tumor tissue in the distant site T2. The large number of M2-like macrophages will protect cancer cells at the distant tissue T2. The M2-like macrophages will cripple immunity against the metastasis cancer. The CNS does everything to promote the metastasis as it did to promote the primary tumor.
Like learning any skills, the CNS memory and skills will improve with time because its state memory can be reinforced by its existence, and the reuse of the CNS skill also improves the CNS’s ability to promote the deviated B&C processes in support of malignancy. By using acquired skills, the CNS causes the body to conduct all remodeling activities to create another masterpiece cancer at much shorter time. The CNS adaptive changes are responsible for increasing malignancy. Time windows for the first, the second, the third and the forth cancer may look like 10 to 50 years, 3 years, 1 year, and 6 months. Cancer may erupt in a single site in the first time, two or more site in the second time, multiple sites in the third time, and the whole body in fourth time
The CNS Protective Roles Explain Controversial Phenomena
We will apply the CNS roles to interpret conflicting or controversial phenomena such as re-population of cancer cells after cancer treatments, increasing cancer malignancy, aging-related cancer occurrence pattern, adverse impacts of chronic stress, and adverse impacts of systemic inflammation on cancer outcomes, etc.
New Evidence on Exercise’s Benefits
We showed that exercise and cancer growth share same B&C processes. Exercise can influence CNS signal exchange efficiency which plays a crucial role in controlling cancer growth. It was found that engaging in exercise following the diagnosis of cancer has a great protective effect against cancer-specific mortality, cancer recurrence, and all-cause mortality, based on the 11 meta-analyses 55. Specifically, superior levels of exercise following a cancer diagnosis were associated with a 28%–44% reduced risk of cancer-specific mortality, a 21%–35% lower risk of cancer recurrence, and a 25%–48% decreased risk of all-cause mortality. Such great benefits can be explained by exercise’s roles of influencing B&C processes through the CNS as shown in Figure 1. Exercises can slowly reduce the deviated B&C processes to ones that do not support cancer proliferation.
Systemic Inflammation
It is well known that systemic inflammation promotes cancer growth 67 by a tumor-extrinsic mechanism. In surgical wounded mice, inflammatory monocytes, the precursors of TAMs, are mobilized systemically in response to surgical wounding, increase their availability for recruitment into tumors. The authors suggested that TAMs may promote tumor outgrowth by countering T cell–mediated growth restriction. They found that PD-L1 expressed by the large number of TAMs deactivated cytotoxic T cells and thus promoted tumor growth. The effect of the inflammation-induced monocytes can be explained in light of Figure 3. Before surgical wound was inflicted, the CNS of the mouse acquired state information on its systemic inflammation, and the severe systemic inflammation caused by the surgical wound caused a big difference between current inflammatory state and the non-inflammation state reflected in the CNS memory. Therefore, the CNS attempts to reduce inflammatory level by altering macrophages species or deactivating M1-like species. Immune suppression is an expected action of the CNS in response to the lasting inflammation.
Cancer Develops Resistance to Cancer Drugs
Cancer drug resistance can be attributed to drug inactivation, drug target alteration, drug efflux, DNA damage repair, cell death inhibition, EMT, inherent cell heterogeneity, epigenetic effects, or any combination of these mechanisms 56. After a drug is used for some time, cancer cells population will decline as a result of drug action. Mitigating or eliminating drug effects is an inherent ability of living organisms to defeat the drug effects. Such an ability was developed in evolution. The CNS must do everything that it can to resist changes in state. If the body is unable to reach a pivotal point of both reducing cancer cells and resetting the CNS state memory, the CNS does as much as it could to help cancer cells to survive. If some cancer cells have been killed, the CNS attempts to restore lost cancer cells and thus encourages cancer repopulate. Compared with cell mutant selection, the CNS may play even a bigger role in the development of drug resistance.
The Role of Chronic Stress in Promoting Cancer
Sloan et al12 used a mouse model to study stress effects and found that chronic stress increased a metastasis of primary breast tumor cells to distant tissues by 38-fold versus controls as indicated by luciferase signal. Stress increased metastasis in clinically relevant tissues, with a 37-fold increase in the lung and a 67% increase in the lymph nodes. It was further found that stress-induced recruitment of immune cells was specific to macrophages. These effects were mediated by β-adrenergic signaling, which increased the infiltration of CD11b + F4/80 + macrophages into the primary tumor and thereby induced a prometastatic gene expression signature accompanied by indications of M2 macrophage differentiation.
Chronic stress triggers changes in brain structure, including differences in the volume of gray matter versus white matter, as well as the size and connectivity of the amygdala. Such changes may impair CNS capacity for storing state memory. When the CNS is overloaded by activities caused by chronic stress, the CNS’ function of regulating the body's state is compromised. In addition, β-adrenergic pathway on stromal cells is used in promoting cancer survival, growth and metastasis.
The CNS roles explain how chronic stress affects cancer outcomes by an additional new mechanism. Chronic stress interferes with the CNS roles by overloading signal transmission along hypothalamus and emotion-sensitive regions and thus interfere with the comparison mechanism. In an attempt to repair the “unhealed wound,” the CNS suppresses the immune system, up-regulate β-adrenergic signaling path, orchestrates bone marrows to generate more monocytes to be recruited into the primary site and other distant sites, causes macrophages to switch from M1-like types to M2-like types in both the primary and metastatic sites, and differentiate the monocytes into M2-like macrophages. The system-wise changes thus result in immunosuppression and promote cancer proliferation.
Tumor Cell Re-population After Radiotherapy
Tumor cells re-population plays a major role in the response of tumors to radiotherapy or chemotherapy. Although overall tumor response rates associated with paclitaxel and platinum range from 70% to 80%, 50%–75% of individuals relapse within 18 months after completing a first-line therapy 57. The mechanism of tumor cell re-population was unknown, and re-population cannot be simply caused by the greater availability of oxygen and nutrients resulting from the reduction in tumor mass. After a large number of cancer cells have been destroyed, the CNS attempts to restore the existing state by sending the same regulatory signals to the tissue where the cancer once situates. The CNS will promote the B&C processes in favor of restoring the prior cancer-promoting state. It will try to restore the attributes of the old metabolic pathways, old structural features, old signals-exchanging patterns, and old immune responsive levels. A sharp rise of cancer cells is natural and proper response of the CNS, which is driven by state memory.
Cancer Cell Re-population After Induction Chemotherapy
For patients with stage III non-small cell lung cancer treated with induction chemotherapy, delayed initiation of subsequent radiotherapy (RT) may allow for re-population in the interval between the induction chemotherapy and the subsequent radiotherapy 58. This is the most typical cancer cell re-population caused by the CNS. In this case, an induction chemotherapy is relatively short, and thus the CNS has a strong tendency to use its regulatory action to restore the prior cancerous state as long as the body has required biological resources. It is natural that a delay will result in rapid rise of cancer cell population.
Cancer Fast Returns after Surgery
Although some cancers recur many years after tumor resection, a substantial fraction of patients develop overt metastases relatively soon after resection of their primary tumors 59, 60, 61. These patients are represented in a sharp rise in the risk of distant recurrence that begins 6 months after surgery and peaks 6 to 12 months later. Slow cancer returns may be caused by altered lifestyles, diets and emotional management that can alter tissue ecosystem by restricting required resources for cancer growth. The cancer return peak of 6 to 12 months seems to be largely controlled by the CNS's regulatory actions and the minimum time for creating enough cancer cells.
B Cells Suppression Caused by Chemotherapy
Many studies have reported effects of chemotherapy on lymphocytes in breast cancer patients during the therapy itself or up to 3 months after the last chemotherapy cycle, with a consensus that chemotherapy reduces circulating lymphocyte levels. A study 62 tried to understand the longer term's impact of chemotherapy, and found that patients receiving epirubicin and cyclophos-phamide EC or 5-flurouracil, epirubicin and cyclophosphamide FEC showed significantly greater B cell depletion compared to the EC+TAX (e.g., 2 EC cycles followed by further cycles of the taxane, docetaxel) group at 2 weeks after treatment (depleted to 3% vs 8% respectively). The EC/FEC group, who suffered the greatest depletion, recovered B cells significantly more quickly than the EC+TAX group, with the difference between the groups reversed and significant at both 6 months and 9 months.
The recovery of the immune system is a manifestation of the roles of the CNS. The recovery pattern would depend on the CNS state memory, original immune cells mixture, effects and duration of chemotherapy, and biological resources in support of the recovery. The general trend is that the types of immune cells with greatest depletion will recover more. Certain changes caused by chemotherapy may prevent the state going back to what the CNS attempts to restore. Thus, the final state is a perturbed immune system which is as close as what the CNS tries to restore.
Cellular Memory (The Body's Memory)
Cui et al63 found that the recurrence of ovarian cancer may be linked to cytotoxin chemotherapy drugs that induce PGE 2 production, despite the chemotherapy is used to kill tumor cells. They found that cleaved caspase 3 can results in the release of arachidonic acid (AA) from membrane phospholipids, which ultimately triggers production of the growth signal prostaglandin E2 (PGE 2). Both AA and PGE 2 can stimulate cell proliferation and tumor growth. Therefore, they suggested that caspase 3 activation ultimately lead to cancer recrudescence through the AA metabolic pathway. The experiment was done with a Transwell system for co-cultures of SKOV3 cancer cells, and thus the CNS does not control the tissue. Instead, the cellular behaviors are controlled by genetic and epigenetic changes that can persist in cells in a culture. The finding cannot be applied to real humans where the CNS controls cancer growth. In vitro, due to lack of CNS regulations over the tissue ecosystem, other pathways or biochemical steps required for cell apoptosis may be impaired so that caspase 3 release appears to be an apparent step for promoting cancer recrudescence. Caspase 3 concentration may be elevated due to impaired or blocked downstream apoptosis steps. In real humans, ovarian cancer cell re-population is most probably induced by the CNS's regulatory signals. If the chemotherapy had been used for a sufficiently long time, the CNS might have attempted to protect the state. The patients in the Cui et al study received two to four short-course regimens of chemotherapy (2–4 months) and it was unlikely that the state memory could be reset in such a short time. It is expected that, upon ending chemotherapy, the CNS attempts to restore the prior-treatment state which is characterized with a low activity of apoptosis. Thus, we believed that Caspase 3 release cannot be the full cause for cancer cell re-population in humans. Instead, cancer re-population is a typical rebound driven by the CNS memory.
Other Chronic Diseases
The CNS roles satisfactorily explain that chronic diseases, even after cured, have strong tendency to return. The body favors regaining lost weight after losing weight; high blood pressures are difficult to manage, and metabolic syndrome are hard to fix due to the CNS’s effort to restore prior body states.
Mysteries of Ancient Healing Exercises
We could not produce suitable evidence from ancient medical systems. Before modern medicine arrived, every medical system in the world used the holistic model which includes mind as part of cure. In China, use of exercises to train mind can be found in every aspect of culture. While current medical model ignores such evidence, their probative value is not any less. Support for the CNS roles can be “experienced” by certain people who are able to pay subtle attention to inner health condition.
Discussion
New Strategies for Fighting Cancer
A best strategy implied from the CNS roles is preventing cancer before the cancer has won the status of CNS protection. When a cancer has fully grown, the cancer has caused the CNS to flip its role from destroying the tumor to protecting/remolding the tumor, a cure must be a comprehensive program with multiple components. One strategy is retraining the CNS and strengthening the signal exchanging efficiency so that the CNS will not keep getting false “insufficient growth” signals. If the CNS can acquire sufficiently strong growth signals from the cancer-residing tissue, it will attenuate, down scale, or even stop its remodeling activities and change neuronal signals for controlling TAMs. Restoring the immune system and changing CNS signals should be the primary goal. Doing extensive well designed mind-targeted exercises should be considered as a primary component of cure because it is the only measure that can retrain the CNS functions. The second strategy is controlling diet, nutrition and life-style factors to alter tissue ecosystem properties so that they are close to ones found in evolution. Those properties are changed to be unfavorable to cancer growth. Cancer growth may be slowed, stopped or even reversed only by restricting necessary nutrition/resources, changing multiple health properties simultaneously, creating cancer-hostile tissue ecosystem, etc. An effective treatment program must be maintained in a sufficiently long time to have the CNS memory reset. Since the CNS can be an active promoter of cancer proliferation and metastasis, management of emotion, fears and chronic stress is a central task for fighting cancer. Those factors can affect the CNS through hypothalamus and amygdala 64, management of emotion and fears should be viewed as an indispensable measure for fighting cancer.
Changes Needed in Future Cancer Research
In the entire medical history, the CNS's memory and its regulatory roles were never considered. CNS regulatory role must be addressed in future medical researches. Our findings reveal a fundamental problem in the cancer treatment paradigm. In early times, chemotherapy, radiotherapy and surgeries were used without understanding cancer biology and the CNS's roles. The cancer progressive puzzle is well known but has not been solved. The riddle can be solved by considering the CNS role. A rapid regrowth of cutaneous or pulmonary metastases has been observed 65, 66. This change is characterized by the ratio of the doubling time before treatment to that during the repopulation phase. It was found that the value of this ratio ranged from 2.5 to 5. This is roughly equivalent to 2.5 to 5 times increase in cancer growth rate constant. The large increase in progression speed is attributed to the CNS’s regulatory function in a context when radiotherapy and chemotherapy impair the immune system and raise systemic inflammation. The impacts of surgery demonstrated by Krall et al 67 can be further explained by the CNS roles: A high inflammation level caused by surgical wound would force the CNS to make great effort to remodel the tissue.
The roles of the CNS could cause many past studies to reach different conclusions. Without considering the CNS roles, one could anticipate that blocking adrenergic receptors may prevent cancer from progressing. However, blocking β-adrenergic signaling path will not stop the CNS from attempting to find alternative ways to raise cancer cell growth speeds. We suspect that the CNS uses its own comparative mechanism to decide when the CNS inhibits cancer or protect cancer cells. The switching point must be decided by the CNS because the CNS is only organ that is capable of making such decisions. A large number of factors including systemic inflammation, cancer type and tumor size, CNS communication efficiency, immune cells mixtures, tissue ecosystem, etc. are presumed to influence the switching point. This is why studies reached different conclusions.
Drug treatments can be defeated by the CNS’s role. Beta blockers was believed to stop cancer growth. The latest meta study involving 319,006 patients shows beta blockers have dubious benefits 68. Another meta study similarly found dubious benefits as judged by disease free survival and overall survival in an epidemiological or perioperative setting 69. Use of chemotherapy in treating cancer is proved to be unsuccessful. The complete response rate of chemotherapy for most types of cancer is locked at about 7.4% 70. A systematic evaluation of cancer drug approved by the European Medicines Agency from 2009 to 2013 shows that most cancer drugs entered the market without evidence of benefits on survival or quality of life 71. The complete responses for thyroid cancer treatment are about 2.5% to 3.4% 72. The true benefits of targeted therapies are extending remission of cancer for a few months 73.
What cancer patients want are predictable cures and fair assurance that can alleviate fears and emotional pains. Medical researchers must seek new strategies because the three CNS roles imply that cancer generally cannot be cured by using one or few drugs alone. Different roles of different macrophage species imply the importance of using a holistic approach. We believe that whether macrophages are properly activated or differentiated with right types and proper ratios depend on subtle balances among a large number of factors. If the CNS decides to accept and promote cancer, the CNS will take coherent and concerted actions to protect cancer cells. Future research should try to identify dominant state properties that can be correlated to cancer outcomes.
Medical research methodology should be reconsidered in the following aspects. First, a state disease may be caused by only a small deviation from a disease-free state. A state, which is defined by a large number of B&C pathways, cannot be meaningfully evaluated by cherry-picking a few state properties. Second, given obvious differences in state properties between different persons, treatments cannot be based on measured individual state properties, but must be based on overall state condition. Third, accurate state properties cannot be based on population trials because great differences in state properties among different patients are expected. Forth, in designing studies for understanding effects of diets, lifestyles, and mind regulation, one should consider how they interact with the CNS. Finally, animal models have limited use because animals do not have the CNS comparable to human’s.
Emotion and Exercises play a unique role. Chronic stress and fears can adversely affect cancer outcome 12, 74, 75, 76. The three CNS's roles imply that both emotional management and exercise are very important in fighting cancer. Excessive neuronal signals caused by constant worries, emotional shocks, fears, etc. interfere with the CNS’ regulatory functions. The medical community should develop a treatment paradigm that is able to adequately address patients’ chronic stress and emotional pains. If the CNS regulatory function is erratic, the integrity of tissue cells cannot be maintained. We have shown that exercises can directly modulate baseline B&C processes against the driving forces of chronic diseases. Long-term exercises have great benefits in fighting cancer 55. Exercises in conjunction with emotional management may help the CNS regain a complete control over the cancer-residing tissue. Such measures may cause the CNS to stop its remodeling effort and restore its anti-tumor immunity signals.
Conclusion
Based on facts extracted from the skill-learning model in conjunction of existing knowledge, we have shown that the CNS can store state information on basic B&C processes in tissue cells, use the stored information in regulating the body, and regulate the body by using a comparative mechanism. With the three functions, the CNS maintains health state for a healthy person and the disease state for a diseased person. The mind-body interlock plays a crucial role in maintaining structural and functional stability of the person. While the CNS memory is essential for maintaining health stability, it is the main obstacle to curing state diseases. No chronic diseases can be cured unless the state information in the CNS memory is changed. The CNS plays a crucial role in cancer initiation, progression and metastasis. The CNS is like a double-edged sword: It initially attempts to prevent, inhibit, or slow down cancer progression. However, after the tumor has reached a sufficient size, the dominance of cancer cells forces the CNS to change its roles from inhibiting and killing cancer cells to protecting cancer cells. Cancer cannot be cured without restoring CNS state memory. Measures for restoring CNS state memory include altering CNS memory directly, restricting biological resources for cancer growth on a long-term basis, and altering state properties of cancer. Exercises and emotional management are the most important measures for restoring the CNS state memory.
Funding Statement
The author(s) declared that no grant was used in support of this research project.
Change History
The article was originally posted on the SSRN preprint server on 13 November 2019 and has been amended several times.
References
- 1.Buijs R M, Scheer F A, Kreier F. (2006) Organization of circadian functions: interaction with the body. Prog Brain Res. 153, 341-60.
- 2.Wójcikowski J, Daniel W A. (2011) The role of the nervous system in the regulation of liver cytochrome p450. Curr Drug Metab. 12(2), 124-38.
- 3.Han C, Rice M W, Cai D. (2016) Neuroinflammatory and autonomic mechanisms in diabetes and hypertension. , Am J Physiol Endocrinol Metab 311(1), 32-41.
- 4.Brydon L, Magid K, Steptoe A. (2006) Platelets, coronary heart disease, and stress. , Brain Behav Immun 20, 113-119.
- 5.Sundquist J, Li X, Johansson S E, Sundquist K. (2005) Depression as a predictor of hospitalization due to coronary heart disease. , Am J Prev Med 29, 428-433.
- 6.Nemeroff C B, Musselman D L, Evans D L. (1998) Depression and cardiac disease. Depress Anxiety. 8(1), 71-79.
- 7.Kiecolt-Glaser J K, Preacher K J, MacCallum R C. (2003) Chronic stress and age-related increases in the proinflammatory cytokine IL-6. Proc Natl Acad Sci USA 100, 9090-9095.
- 8.Wraith D C, Nicholson L B. (2012) The adaptive immune system in diseases of the central nervous system. , J Clin Invest 122(4), 1172-1179.
- 9.Kiecolt-Glaser J K, Marucha P T, Malarkey W B. (1995) Slowing of wound healing by psychological stress. , Lancet 346, 1194-1196.
- 10.Segerstrom S C, Miller G E. (2004) stress and the human immune system: a meta-analytic study of 30 years of inquiry. , Psychological Bulletin 130(4), 601-630.
- 11.McDonald P G, Antoni M H, Lutgendorf S K. (2005) A biobehavioral perspective of tumor biology. , Discovery Medicine 5(30), 520-526.
- 12.Sloan E K, Priceman S J, Cox B F. (2010) The sympathetic nervous system induces a metastatic switch in primary breast cancer. Cancer Research. 70(18), 7042-7052.
- 13.Kleemeyer M M, Polk T A, Schaefer S. (2017) . Exercise-Induced Fitness Changes Correlate with Changes in Neural Specificity in Older Adults. Front Hum Neurosci 11, 123.
- 14.Lumen.Boundless Anatomy and Physiology, Control of Muscle Tension, Force of Muscle Contraction. https: //courses.lumenlearning.com/boundless-ap/chapter/control-of-muscle-tension/. Last
- 15.Booth F W, Roberts C K, Laye M J. (2012) Lack of exercise is a major cause of chronic diseases. , Compr Physiol 2, 1143-1211.
- 16.Prehn R T.1994;Cancers beget mutations versus mutations beget cancers. , Cancer Res 54, 5296-5300.
- 19.Wang T L, Rago C, Silliman N, Ptak J. (2002) Prevalence of somatic alterations in the colorectal cancer cell genome. Proc Natl Acad Sci USA 99, 3076-80.
- 20.Wood L D, Parsons D W, Siân Jones. (2007) The genomic landscapes of human breast and colorectal cancers. , Science 318(5853), 1108-1113.
- 21.Jones S, Chen W-D, Parmigiani G. (2008) Comparative lesion sequencing provides insights into tumor evolution. Proc Natl Acad Sci USA 105, 4283-4288.
- 22.Hochberg M E, Noble R J. (2017) A framework for how environment contributes to cancer risk. , Ecology Letters 20, 117-134.
- 24.Khasraw M, Posner J B. (2010) Neurological complications of systemic cancer. , Lancet Neurol 9, 1214-1227.
- 25.Toothaker T B, Rubin M. (2009) Paraneoplastic neurological syndromes: a review. , Neurologist 15, 21-33.
- 26.Mravec B, Gidron Y, Hulin I. (2008) Neurobiology of cancer: Interactions between nervous, endocrine and immune systems as a base for monitoring and modulating the tumorigenesis by the brain. Semin Cancer Biol. 18, 150-163.
- 27.de Visser KE, Eichten A, Coussens L M. (2006) Paradoxical roles of the immune system during cancer development. Nat Rev Cancer. 6, 24-37.
- 28.DeNardo D G, Johansson M, Coussens L M. (2008) Immune cells as mediators of solid tumor metastasis. Cancer Metastasis Rev. 27, 11-18.
- 29.Wu Y, Zhou B P. (2009) Inflammation: a driving force speeds cancer metastasis. Cell Cycle. 8, 3267-3273.
- 30.Solinas G, Marchesi F, Garlanda C. (2010) Inflammation-mediated promotion of invasion and metastasis. Cancer Metastasis Rev. 29, 243-248.
- 31.Nguyen D X, Bos P D, Massague J. (2009) Metastasis: from dissemination to organ-specific colonization. Nat Rev Cancer. 9, 274-284.
- 32.Sung S Y, Hsieh C L, Wu D. (2007) Tumor microenvironment promotes cancer progression, metastasis, and therapeutic resistance. Curr Probl Cancer. 31, 36-100.
- 33.Calorini L, Bianchini F. (2010) Environmental control of invasiveness and metastatic dissemination of tumor cells: the role of tumor cell-host cell interactions. Cell Commun Signal. 8, 24.
- 34.Palm D, Entschladen F. (2007) Neoneurogenesis and the neuroneoplastic synapse. Prog Exp Tumor Res. 39, 91-98.
- 36.Albo D, Akay C L, Marshall C L. (2011) Neurogenesis in colorectal cancer is a marker of aggressive tumor behavior and poor outcomes. , Cancer 117, 4834-4845.
- 38.Ayala G E, Dai H, Powell M. (2008) Cancer-related axonogenesis and neurogenesis in prostate cancer. Clin Cancer Res. 14, 7593-7603.
- 40.Canaani J, Kollet O, Lapidot T. (2011) Neural regulation of bone, marrow, and the microenvironment. Front Biosci. 3, 1021-1031.
- 41.Benestad H B, Strom-Gundersen I, Iversen P O. (1998) No neuronal regulation of murine bone marrow function. , Blood 91, 1280-1287.
- 42.Artico M, Bosco S, Cavallotti C. (2002) Noradrenergic and cholinergic innervation of the bone marrow. Int J Mol Med. 10, 77-80.
- 43.Imai S, Tokunaga Y, Maeda T. (1997) Calcitonin gene-related peptide, substance P, and tyrosine hydroxylase-immunoreactive innervation of rat bone marrows: an immunohistochemical and ultrastructural investigation on possible efferent and afferent mechanisms. J Orthop Res. 15, 133-140.
- 45.Lin W W, Karin M. (2007) A cytokine-mediated link between innate immunity, inflammation, and cancer. , J Clin Invest 117, 1175-1183.
- 46.Karin M, Greten F R, kappa N F. (2005) linking inflammation and immunity to cancer development and progression. , Nat Rev Immunol 5, 749-759.
- 47.Dvorak H F. (1986) Tumors: wounds that do not heal. Similarities between tumor stroma generation and wound healing. , N Engl J Med 315, 1650-9.
- 49.Xue J, Schmidt S V, Sander J.Transcriptome-based network analysis reveals a spectrum model of human macrophage activation. , Immunity 40(2), 274-288.
- 50.Huang Y C, Feng Z P. (2013) The good and bad of microglia/macrophages: new hope in stroke therapeutics. Acta Pharmacol Sin. 34(1), 6-7.
- 51.Aras S, Zaidi M R. (2017) TAMeless traitors: macrophages in cancer progression and metastasis. , British Journal of Cancer 117, 1583-1591.
- 52.Noy R, Pollard J W. (2014) Tumor-associated macrophages: from mechanisms to therapy. Immunity. 41(1), 49-61.
- 54.Carabotti M, Scirocco A, Maselli M A, Severi C. (2015) The gut-brain axis: Interactions between enteric microbiota, central and enteric nervous systems. , Ann. Gastroenterol 28, 203-209.
- 55.Cormie P, Zopf E M, Zhang X, Schmitz K H. (2017) The Impact of Exercise on Cancer Mortality, Recurrence, and Treatment-Related Adverse Effects. Epidemiologic Reviews. 39(1), 71-92.
- 56.Housman G, Byler S, Heerboth S H. (2014) Drug Resistance in Cancer: An Overview. , Cancers 6, 1769-1792.
- 57.Salani R, Backes F J, Fung M F.Posttreatment surveillance and diagnosis of recurrence in women with gynecologic malignancies: Society of Gynecologic Oncologists recommendations. , Am J Obstet Gynecol 204(6), 466-478.
- 58.Chen C P, Weinberg V K, Jahan T M. (2011) Implications of Delayed Initiation of Radiotherapy Accelerated Repopulation after Induction Chemotherapy for Stage III Non-small Cell Lung Cancer. Journal of Thoracic Oncology. 6(11), 1857-64.
- 59.Cheng L, Swartz M D, Zhao H.2012; Hazard of recurrence among women after primary breast cancer treatment—A 10-year follow-up using data from SEER-medicare. Cancer Epidemiol. Biomarkers Prev. 21, 800-809.
- 60.Colleoni M, Sun Z, Price K N. (2016) Annual hazard rates of recurrence for breast cancer during 24 years of follow-up: Results from the international breast cancer study group trials I to V. , J. Clin. Oncol 34, 927-935.
- 61.Hüsemann Y, Geigl J B, Schubert F. (2008) Systemic spread is an early step in breast cancer. , Cancer Cell 13, 58-68.
- 62.Verma R, Foster R E, Horgan K. (2016) Lymphocyte depletion and repopulation after chemotherapy for primary breast cancer. , Breast Cancer Research 18, 10.
- 63.Cui L, Zhao Y, Pan Y. (2017) Chemotherapy induces ovarian cancer cell repopulation through the caspase 3-mediated arachidonic acid metabolic pathway. Onco Targets Ther. 10, 5817-5826.
- 64.Phelps E A, LeDoux J E. (2005) Contributions of the Amygdala to Emotion Processing: From Animal Models to Human Behavior. , Neuron 48, 175-187.
- 65.Tubiana M. (1988) Repopulation in human tumors. A biological background for fractionation in radiotherapy. , Acta Oncol 27, 83-8.
- 66.Tubiana M. (1989) Tumor Cell Proliferation Kinetics and Tumor Growth Rate. , Acta Oncologica 28(1), 113-121.
- 67.Krall J A, Reinhardt F, Mercury O A. (2018) The systemic response to surgery triggers the outgrowth of distant immune-controlled tumors in mouse models of dormancy. Sci Transl Med. 10(436), 3464.
- 68.Na Z, Qiao X, Hao X. (2018) The effects of beta-blocker use on cancer prognosis: a meta-analysis based on 319,006 patients. OncoTargets and Therapy. 11, 4913-4944.
- 69.Yap A, Lopez-Olivo M A, Dubowitz J. (2018) Effect of beta-blockers on cancer recurrence and survival: a meta-analysis of epidemiological and perioperative studies. , Br J Anaesth 121(1), 45-57.
- 70.Ashdown M L, Robinson A P, Yatomi-Clarke S L. (2015) Chemotherapy for Late-Stage Cancer Patients: Meta-Analysis of Complete Response Rates. 4, 232.
- 71.Davis C, Naci H, Gurpinar E. (2017) Availability of evidence of benefits on overall survival and quality of life of cancer drugs approved by European Medicines Agency: retrospective cohort study of drug approvals. 359, 4530.
- 72.Albero A, Lopéz J E, Torres A. (2016) Effectiveness of chemotherapy in advanced differentiated thyroid cancer: a systematic review. Endocr Relat Cancer. 23(2), 71-84.
- 73.Maeda H, Khatami M. (2018) Analyses of repeated failures in cancer therapy for solid tumors: poor tumor-selective drug delivery, low therapeutic efficacy and unsustainable costs. , Clin Transl Med 7, 11.
- 74.Moreno-Smith M, Lutgendorf S K, Sood A K. (2010) Impact of stress on cancer metastasis. , Future Oncology 6(12), 1863-1881.