
Abstract
Background and Objective:
Behavioral procedures have proven to be effective with elderly adults in nursing home. The purpose of this study was to evaluate the effectiveness of a shaping procedure as a means of increasing writing performance. More specifically, our aim was to reeducate a motor behavior in a patient for whom the behavior was no longer present.
Materials and Methods:
The participant was an elderly (76-year-old) who had sequelae from a cardiovascular accident since 2011, and was asked to write some selected words. Data were collected though face-to-face interviews then analyzed using cotation methods.
Results:
The shaping and chaining procedures were efficient and performance of writing increased, even for infrequent words.
Conclusion:
Increasing writing performance is possible for the elderly people, even if they have suffered from cardiovascular accidents in the past. Here we used a successful brief shaping procedure to enhance quickly that ability.
Author Contributions
Academic Editor: Roman Kireev, PhD, Senior Researcher
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Charlotte Renaux, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Concerns about care for the elderly raise a societal issue. In 2003, cardiovascular diseases caused 17 million of deaths, one third of all deaths in the world1. Caring for patients who have had a cardiovascular accident is needed to prevent another accident, caused by the immediate and long term clinical consequences of the stroke2. Higher-order cognitive abilities like calculation or naming are considered as having an important role to play in stroke rehabilitation3. Moreover, the use of intensive and multidisciplinary rehabilitation exercises implemented by physiotherapists, dieticians and speech therapists, has been shown to positively influence functional outcomes in a large-scale clinical research investigating 1588 stroke patients4. New technologies are also being used to improve the efficacy of rehabilitation. Indeed, virtual reality interface5 and EEG brain machine interface6 have been shown helpful for the implementation of rehabilitation exercises and may boost the recovery of stroke patients.
In Applied behavior analysis, only 1.67% of current publications adressed aging issues7 despite its effectiveness in the high-order cognitive abilities and the management of behavioral disorders. Behavioral procedures have proven to be effective with elderly adults in nursing home, moreover by its easy implementations. Indeed, such behavioral procedures can be quickly implemented by experts and non-experts following protocols. Applied behavior analysis focuses on the target behavior and its natural reinforcers (e.g. social reinforcers). Some author’s conducted a functional analysis and a differential reinforcement procedure to decrease problem behaviors of dementia patients, such as disruptive vocalizations or wandering8. Others showed the utility of using non-contingent reinforcement, with the use of music, to treat disruptive vocalizations in dementia patients9. Unlike previous articles, some authors addressed skills building and used an antecedent intervention in order to increase activity attendance and engagement in individuals with dementia10.
The purpose of the current study was to use a shaping procedure to improve the writing ability of an elderly patient with sequelae caused by a cardiovascular accident. Our aim was to reeducate in a limited amount of time (i.e. 26 days) a motor behavior in a patient for whom the behavior was no longer present (i.e. previously learned behavior which appeared to be extinct).
The shaping procedure consists of reinforcing the production of gradually changing response classes; each response class being a successive approximation toward a target behavior11. This procedure is appreciated for its positive approach. Indeed, the shaping procedure involves a slow stepwise procedure that builds on the individual’s current repertoire until more complex targeted responses can be emitted. The extent of progress of the patient determines the amount of time spent at each step, thus behavioral requirements are always only slightly above behavioral capacity, and likelihood of failure is reduced12. For example, a shaping procedure has been applied in a medical rehabilitation setting where an elderly patient had to learn to walk independently after injuring her hip. She first learnt to stand between parallel bars, then to use the parallel bars to help support her while she walks, then to use a walker to support her as she walks, then to use crutches to walk and finally to walk independently13. Using such a step-by-step procedure not only got the patient back to walking, it also generated a positive interaction between the patient and the therapists, and the patient developed a keen interest in walking.
We thus implemented a shaping procedure that could be easily used by the different staff members (i.e. experts and non-experts psychologists). We applied the shaping procedure’s stepwise approach built on the word frequency effect.
In psycholinguistic, the word frequency effect refers to the finding that high frequency words are more easily identified than low frequency words14. In this experiment, we used words of 100%, 75%, 50%, 25% frequency and logatomes (i.e. non-existent words). Our hypothesis predicts that the more the patient writes chains of letters, the better his performance will be.
Method
Participant
The participant, Mrs. L., is a 76-year-old French woman hospitalized in a long-term care facility (Centre Long Séjour of Boulogne-sur-Mer, France). Three years prior to this study, Mrs. L. was admitted after a cardiovascular accident in which she completely lost her speaking skills (i.e. vocal and writing verbal behaviors). Since the summer 2013, Mrs. L. had been treated by a speech therapist but still suffered from semantic paraphasia (e.g. anomia). Mrs. L. read and signed an informed consent form prior to the procedure. The procedure had been approved by the long-term care facility (Centre Long Séjour of Boulogne-sur-mer, France), and was applied for 26 sessions (i.e. 5 days per week during one month) by two masters’ students supervised by the authors.
Setting and Material
Before each session, ten untested words were randomly selected from the Ministry of National Education’s websitea. This website provides a classification of French words from the most commonly used to the least commonly used. For the 3-month follow-up, logatomes were retrieved from a logatome generator of University Paris Descartes, Franceb. The aim of creating logatomes was to use 0% frequency words with already trained chains of letters.
Interventions were conducted with the two experimenters in the Mrs. L.’s room, where all necessary equipment was brought as rating scales, tally counters and a watch.
Each session consisted of a written task followed by a reading time. During the writing task, a sheet of paper on a clipboard with a pen were used by Mrs. L. Then the favorite book used was picked in the facility’s library: Mon bel aristocrate (Heather, 1983).
Response Measurement and Interobserver Agreement
The behavior targeted was to write a word correctly, more precisely it was defined as the point-to-point correspondence between a request and the permanent product. The number of correct responses was collected by ten-trial sessions, and converted into a percentage of correct responses. The criterion to increase words frequency was two consecutive sessions at 80%. The interobserver agreement was calculated in that way: Number of Agreements/(Number of Agreements + Disagreements) x 100.
Procedure
Baseline/Pretraining.
The experimenter asked Mrs. L to write the target words. If Mrs. L did not answer, no guidance was provided and the next instruction was presented. Otherwise, if Mrs. L. wrote it, the next instruction was presented with minimal feedback (e.g. “OK”). Words were classified according to their frequency: 100%, 50% and 0%.
Treatment.
Experimenters provided Mrs. L. with a sheet of paper on a clipboard with a pen. Each session consisted of 10 new words (i.e. avoiding training effect on specific words). These new words were retrieved from the National Education Website. Instructions were given in the form of a question (e.g. “Can you write the word Jardinc?”). If the target word was correctly written, the experimenter socially reinforced, and 30 seconds were added to the reinforcing activity’s time. On the other hand, a misspelled word or no response within 5 seconds of the instruction resulted in a vocal prompt being delivered. The experimenter would spell out loud each letter of the target word during vocal prompting. As mentioned above, prompting was delivered using a constant time delay of 5 seconds.
The reinforcer was a reading activity following the writing task. Mrs. L. was provided with two minutes of reading time, with the possibility to earn 30 additional seconds for each word written correctly written. In order to gradually increase the difficulty of the experiment, a shaping procedure was implemented. The first words to be presented were high frequency words (100%), then words that were less frequently encountered (75% frequency), then words that were even less frequently encountered (50% frequency), and so forth until the 25% frequency words could be presented.
Follow-up/Post-training.
Three months after the termination of the intervention, the experimenters proceeded to a follow-up study. The follow up was led in the same manner as the Baseline sessions, except that the 0% frequency words were replaced by non-words. If there is an improvement in the performance for non-words, then it would confirm our hypothesis: the more the client writes specific sequences of letters, the better the overall results.
Results
Records were collected by experimenters after each session (i.e 5 sessions per week during one month; then three months later for the follow-up). Figure 1 showed the quick effect of the shaping procedure. The criterion to increase words frequency was two consecutive sessions at 80%. In 4 sessions Mrs. L. was able to write frequent words (100% word frequency); 4 sessions later she reached the 75%-word frequency criterion, and 15 sessions later mastery criterion was achieved. The results indicate that the writing performance has been considerably enhanced after the 26 training sessions.
Figure 1.Detailed percentages of correctly written words according to word frequency during pre-training/baseline(BL), training (T) and 3 months after training (3-FU).
Figure 2 displays the results of the probes before and after training. During baseline, percentage of correctly written words were high (M=85%) for 100%, average (M=50%) for 50% and low (M=15%) for 0%-word frequency. Following the termination of the shaping procedures (see Figure 1 for more details), which reinforced approximations of the target stimuli (i.e. 0%-word frequency), performance improved. As shown in the right-hand side of Figure 2, percentages increased to 100%, 57,15% and 60% respectively for each of the three frequencies.
Figure 2.Percentage of correctly written words according to the different word frequencies (100, 50 and 0%) for the sessions before and after the training.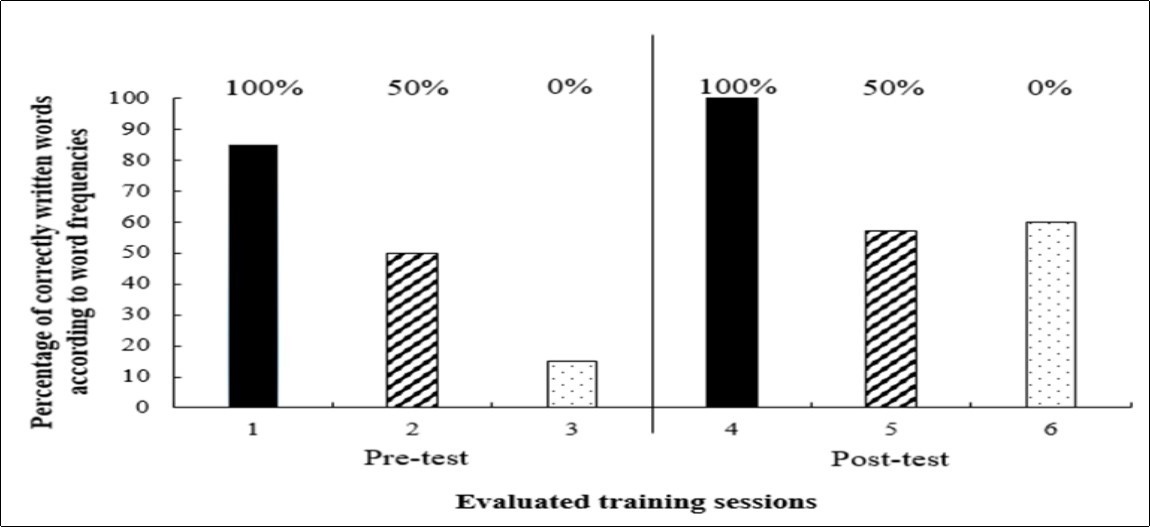
Figure 3 compares the writing performance with regards to existing words known as infrequent as well as for non-words created from letters chaining which were trained during the shaping procedure. The performance increased from 15% in the baseline session to 60% in the follow-up session, which shows that writing ability is not a function of word frequency. Indeed, if it had been the case, Mrs. L. wouldn't have been able to write logatomes. Rather, since new responses appeared, the shaping procedure seems to have been efficient. By reinforcing approximations present in Mrs. L's behavioral repertoire (i.e. relatively frequent learned words), the ability to write non-existent words which consisted of the same letters emerged.
Figure 3.Percentage of correctly written 0% frequency words in pre-training/baseline and after the training (3 months later).
Discussion
Those results show that learning to write is possible for the elderly, even if they have suffered from accidents in the past (i.e. in this case, a cerebral accident). Other studies have proved that adaptation is feasible for several individuals in altered environmental conditions. Eye-hand coordination in prism paradigm with typical individuals has been tested and showed a stable adaptation15. In addition, aphasia produced by traumatic brain injury has been remediated with two individuals (33 and 40 years old) brain damaged for a dozen years16. In that previous study, tact, mand and intraverbal training procedures were derived from Skinner’s17 analysis of verbal behavior. The ability to name stimuli which seemed to be “forgotten” was also demonstrated with a prompting procedure for patients diagnosed with Alzheimer’s disease18. In this case report, writing words of 0% frequency was a hard task for Mrs. L at the beginning of the procedure. In a 3-months follow-up, Mrs. L. was still able to write logatomes. Although this is a small task in an elderly patient, the results are interesting because they are socially important.
Conclusion
The shaping and chaining procedures used were efficient and writing performance improved in 26 days, even for infrequent words. In this case report we demonstrate the feasibility of behavioral procedures, which can be applied by everyone in a short-time application.
The applied dimension of behavior analysis is centered on the target behavior and its importance to the individual19, 20. This study was carried out following a personal request of the patient in order to improve her participation in the workshops and cognitive stimulation training offered by the facility. These workshops are considered as fundamental in reducing risk of cognitive decline21. A further investigation would be to implement a procedure such as presented in this article with others patients with dementia. Our results should be regarded as a starting point for further research whereby the protocol of investigation employed in the present paper would be implemented with patients with dementia, such as Alzheimer’s disease.
References
- 1.Mackay J, Mensah G A.(2004).World Health Organization&Centers for Disease Control and Prevention(U.S.).The atlas of heart disease and stroke. Geneva:World Health Organization.
- 2.Bamford J, Dennis M, Sandercock P, Burn J, Warlow C. (1990) The frequency, causes and timing of death within 30 days of a first stroke: the Oxfordshire Community Stroke Project. , Journal of Neurology, Neurosurgery and Psychiatry 58, 824-829.
- 3.Galski T, R L Bruno, Zorowitz R, Walker J. (1993) Predicting length of stay, functional outcome, and aftercare in the rehabilitation of stroke patients. The dominant role of higher-order cognition. , Stroke 24(12), 1794-1800.
- 4.Imura T, Nagasawa Y, Fukuyama H, Imada N, Oki S et al. (2017) Effect of early and intensive rehabilitation in acute stroke patients: retrospective pre-/post-comparison in Japanese hospital. Disability and Rehabilitation. 1-4.
- 5.D J Berger, d’Avella A. (2017) Towards a Myoelectrically Controlled Virtual Reality Interface for Synergy-Based Stroke Rehabilitation. In Converging Clinical and Engineering Research on Neurorehabilitation II.Springer International Publishing 965-969.
- 6.Sarasola-Sanz A, López-Larraz E, Irastorza-Landa N, Klein J, Valencia D et al. (2017) An EEG-Based Brain-Machine Interface to Control a 7-Degrees of Freedom Exoskeleton for Stroke Rehabilitation. In Converging Clinical and Engineering Research on Neurorehabilitation II.Springer International Publishing 1127-1131.
- 7.M A Trahan, Kahng S, A B Fisher, N L Hausman. (2011) Behavior-analytic research on dementia in older adults. , Journal of Applied Behavior Analysis 44(3), 687-691.
- 8.K J Dwyer-Moore, M R Dixon. (2007) Functional analysis and treatment of problem behavior of elderly adults in long-term care. , Journal of Applied Behavior Analysis 40, 679-683.
- 9.J A Buchanan, J E Fisher. (2002) Functional assessment and non-contingent reinforcement in the treatment of disruptive vocalizations in elderly dementia patients. , Journal of Applied Behavior Analysis 35, 99-103.
- 10.Brenske S, E H Rudrud, K A Schulze, J T Rapp. (2008) Increasing Activity Attendance and Engagement in Individuals with Dementia Using Descriptive Prompts. , Journal of Applied Behavior Analysis 41(2), 273-277.
- 11.J O Cooper, T E Heron, W L Heward. (2007) Applied behavior analysis, 2nd ed.Upper Saddle River,N.J.:PearsonPrenticeHall.
- 13.G W O’Neil, Gardner R. (1983) Behavioral principles in medical rehabilitation:A pratical guide.Sprinfield, IL:Charles C.Thomas.
- 14.Andrews S, Heathcote A. (2001) Distinguishing common and task-specific processes in word identification: A matter of some moment?. , Journal of Experimental Psychology: Learning, Memory, and Cognition 27(2), 514-544.
- 15.J C Hay, Jr Pick, L H. (1966) Visual and proprioceptive adaptation to optical displacement of the visual stimulus. , Journal of Experimental Psychology 71(1), 150-158.
- 16.Sundberg M L, San Juan B, Dawdy M, Argüelles M. (1990) The acquisition of tacts, mands, and intraverbals by individuals with traumatic brain injury. The Analysis of Verbal Behavior. 8, 83-99.
- 18.Dixon M, J C Baker, K A Sadowski. (2011) Applying Skinner’s analysis of verbal behavior to persons with dementia. , Behavior Therapy 42(1), 120-126.
- 19.Baer D M, Wolf M M, Risley T R. (1968) Some current dimensions of applied behavior analysis. , Journal of Applied Behavior Analysis 1, 91-97.
- 20.Baer D M, Wolf M M, Risley T R. (1987) Some still-current dimensions of applied behavior analysis. , Journal of Applied Behavior Analysis 20, 313-327.
- 21.G E Smith, Housen P, Yaffe K, Ruff R, R F Kennison et al. (2009) A cognitive training program based on principles of brain plasticity: results from the Improvement in Memory with Plasticity‐based Adaptive Cognitive Training (IMPACT). , Study. Journal of the American Geriatrics Society 57(4), 594-603.