Abstract
Background
The COVID-19 pandemic has had significant impact on healthcare worldwide. Surgeons are at increased occupational risk of contracting COVID-19. The impact of the disease on surgical practice will continue to evolve. We assessed the impact of the disease on surgical practice and training in Nigeria.
Method
Survey questionnaire was designed, transcribed to Google form and electronically circulated online to surgeons practicing in Nigeria. Surgeons from various subspecialties from the six regions in Nigeria were included. Survey questions pertaining to pre-COVID-19 era surgical practices, impact on current practice and changes occurring in health facilities during this COVID-19 pandemic. Responses were collated and analyzed statistically.
Results
One hundred and nine (109) surgeons completed the survey, of which 2.8% were women. Majority (68.8%) of the respondents are in the consultant cadre, majority (86.2%) are working in public hospital, 88.1% running their SOPD, 81.7% have isolation wards in their centers, 66.1% have dedicated team for COVID-19 management. Only 48.6% of the frontline health workers have access to personal protective equipment (PPE), and 33.9% had formal training on the use of PPE. Only 11.0% were satisfied with level of preparation of the management. Elective cases were done only in 45% of respondents. 103(94.4 %) confirmed that the numbers of elective cases are less than pre Covid-19 period. Emergency cases were carried out by 93.6% of respondents. Only 1.8% of respondents carried out screening tests for their patients before embarking on emergency surgery.
Conclusion
COVID-19 has led to reduction in surgical outpatients, significant reduction in elective surgeries in Nigeria. Adequate PPE needs to be provided, there should be guidelines for safety for future. There should be adequate preparation should there be any pandemic in the near future.
Author Contributions
Academic Editor: Raul Isea, Fundación Instituto de Estudios Avanzados -IDEA
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2022 Owolabi Dele Ojo, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
The Corona virus infectious disease otherwise called COVID-19 is caused by a novel coronavirus 2 (SARS-CoV-2) formally called 2019 – n CoV, was first identified amid an outbreak of respiratory illness cases in Wuhan City, Hubei Province, China. 1
It was initially reported to WHO on December 31, 2019. On January 30, 2020, the WHO declared the COVID-19 outbreak a global health emergency 2, 3. On March 11, 2020, WHO declared COVID-19 a global pandemic. 4
The illness caused by SAR-CoV2 was recently termed COVID-19 by WHO, the new acronym derived from coronavirus disease 2019. The name was chosen to avoid stigmatizing the virus’s origin in terms of population, geography or animal association. 5, 6On February 11,2020, the coronavirus Study Group of International Committee on Taxonomy of Viruses issued a statement announcing an official designation for the novel virus; severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). 7
This COVID-19 infection is a highly contagious disease from man to man and it has constituted health emergency to the whole world and yet to have a definitive cure. Health workers, including surgeons are not spared in contacting this disease in the course of discharging their duty.
As at 01/05/2020, worldwide, 3,269,667 have tested positive, 1,021,185 recovered and 233,560 deaths. In Nigeria 1,932 tested positive, 319 recovered and 58 deaths. 8. As at 01/05/2020, 113 health workers in Nigeria have contacted the disease in the course of discharging their legitimate duty, Surgeons inclusive.8
Statement of Problem
The practice and lives of health workers including surgeons have been affected in many ways following the emergence of COVID-19 disease in Nigeria. This highly contagious disease has high morbidity and mortality with so many questions left to be answered.
Aims
The aim of this study shall be to determine the impact of COVID-19 pandemic on surgical practice in Nigeria.
Objectives
This study seeks to evaluate the changes occurring in health facilities and the practice by surgeons during the COVID-19 outbreak in Nigeria.
To find out the problems encountered by surgeons as regards surgical practice during this COVID-19 pandemic in Nigeria.
Significant of the Study (Benefits)
This study has not been carried out in this locality; the findings will help suggest ways to mitigate against these problems to institutions and policy makers.
Methodology
This prospective survey was conducted among surgeons in tertiary health-care hospitals in Nigeria. Nigeria has a population of over 200 million and it is divided into six regions or zones (North East, North West, South West, South East, South-South and North central). The instrument of the study was self-administered open-ended questionnaire which was designed using a Microsoft Word Version 10 (Microsoft, Seatle, WA, USA ) and transcribed to Google form. The questionnaire was pretest in three institutions different from our own in order to ensure its reliability. There after it was electronically circulated online to Surgeons (Consultants, Senior Registrar and Registrar) practicing in Nigeria. All the Surgeons in various subspecialties were included in the study. Their consent was sought and also their confidentiality was assured. The self-administered questionnaire consists of forty questions to obtain information on the sociodemographic characteristics of the participants, information relating to their professional experience, hospital setting, outpatients and surgical emergencies/electives, number of surgical cases pre-lockdown and post-lockdown periods were obtained. Availability and use of personal protective equipment’s and hospital infrastructures were also obtained.
Sample Size Determination
A minimum sample size for this study was calculated using the Leslie and Kish formula for sample size determination
N = Z2pq / d2
Where: N= the desired sample size
Z= the standard normal deviation, usually set at 1.96 p= the proportion in the target population estimated to have particular characteristics
Available prevalence of covid -19 patients from target population was
54.6%
q=1.0-p = 1- 0.55= 0.45.
d = absolute deviation or amount of difference allowed between the target and the study population (0.1).
Hence, N =1.962× 0.55 × 0.45/0.12 = 95
Using an attrition rate of 10%, N = 105
Data obtained were recorded and analyzed using SPSS Version 22 (Chicago III. USA) and presented as percentages, tables and charts.
Ethical Clearance
Ethical clearance was obtained from the Ethical Committee of the hospital.
Results
Out of 109 respondents, 106 (97.2%) were males while 3 (2.8%) were females given a female to male ratio of 1:35. The age group 41 -50 years has the highest responses and represents 49.5% of the respondents. Majority (68.8%) of the respondents are in the consultants’ cadre, 18.3% are Senior Registrars while 12.8% were Registrars. Majority (86.2%) are working with public hospitals, 2.8 % with private hospitals while 11.0% are working with both public and private hospitals. See Table 1. The surgical specialty that has highest number of responses was Orthopaedics and trauma in 26.6%, followed by General Surgery in 22.9%. See Figure 1. Majority (88.1%) of the respondents are running SOPD in their various institutions. About 81.7% have isolation wards in their centers. Also 66.1% have a dedicated team for covid-19 management. Only 48.6% of the frontline health workers have access to personal protective equipment (PPE), and 33.9% had formal training on the use of PPE. Only 11.0% were satisfied with level of preparation of the management. Elective cases were done only in 45% of respondents. 103(94.4 %) confirmed that the numbers of elective cases are less than pre Covid-19 period. Emergency cases were carried out by 93.6% of respondents. Only 1.8% of respondents carried out screening tests for their patients before embarking on emergency surgery. See Table 2.
Figure 1.Showing Surgical specialties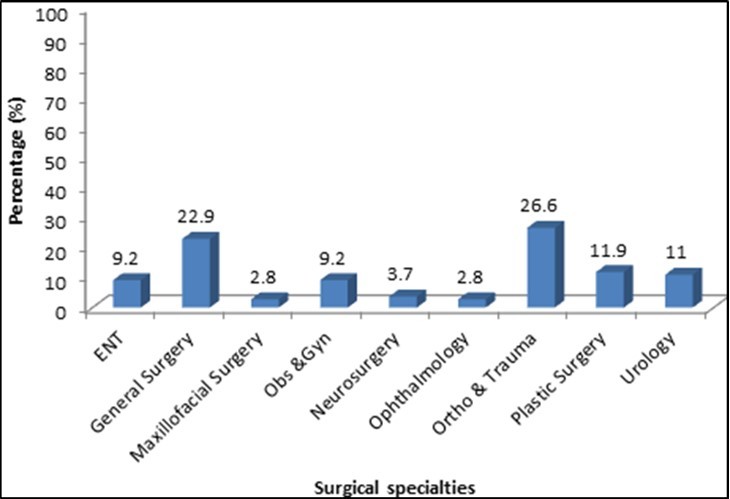
| Parameter | Frequency (n) | Percentage (%) |
|---|---|---|
| Age group (years) | ||
| 21 – 30 | 6 | 5.5 |
| 31 – 40 | 29 | 26.6 |
| 41 - 50 | 54 | 49.5 |
| 51 – 60 | 18 | 16.5 |
| 61+ | 2 | 1.8 |
| Gender | ||
| Male | 106 | 97.2 |
| Female | 3 | 2.8 |
| Cadre of Surgeon | ||
| Consultant | 75 | 68.8 |
| Senior Registrar | 20 | 18.3 |
| Registrar | 14 | 12.9 |
| Year spent in specialty (years) | ||
| 1 – 5 | 28 | 25.7 |
| 6 – 10 | 39 | 35.8 |
| 11 – 15 | 23 | 21.1 |
| 16 – 20 | 9 | 8.3 |
| 20+ | 10 | 9.2 |
| Hospital of Practice | ||
| Public Hospital | 94 | 86.2 |
| Private Hospital | 3 | 2.8 |
| Both | 12 | 11 |
| Parameter/variable/category | Yes (%) | No (%) |
|---|---|---|
| Is your SOPD running? | 96 (88.1) | 13 (11.9) |
| Any Isolation ward | 89 (81.7) | 20(18.3) |
| Any dedicated team for covid -19 | 72 (66.1) | 37(33.9) |
| PPE for frontline health workers | 53(48.6) | 56(51.4) |
| Satisfied level of preparedness | 12(11.0) | 97(89.0) |
| Formal training on infection control | 64 (58.7) | 45(41.3) |
| Formal training on use of PPE | 37(33.9) | 72(66.1) |
| Do you operate elective cases | 49(45.0) | 60(55.0) |
| No of elective cases less than pre Covid-19 | 103(94.4) | 6(5.5) |
| Performing emergency operation | 102(93.6) | 7(6.4) |
| Do you test all emergency cases for Covid-19 | 2(1.8) | 107(98.2) |
Discussion
Coronavirus disease 2019 (COVID-19) is an infectious disease caused by a newly discovered severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). 9. The ongoing pandemic of Coronavirus disease 2019 has rigorous effects worldwide. Immunocompromised patients and people incubating other infections are more vulnerable and prone to COVID-19. COVID-19 pandemic has seriously affected the social as well as economic activities worldwide. Treatment for COVID-19 patients relies mostly on supportive care, mechanical ventilation and/or medication previously employed against other coronaviruses 10. However, surgical cases were also presented during the period. This study aimed to show the effects of COVID-19 on surgical practice in Nigeria. Our study showed that there are more male surgeons than female. This is the usually pattern in most hospital in Nigeria. Consultants’ cadre constitute majority (68.8%) of the doctors that present in the hospital at any given time. As they were supposed to supervise the junior doctors (Residents and Medical Officers) apart from critical decisions that they needed to make. Larger percentages of our respondents were working in the public hospitals. This is so because Nigeria has many hospitals at states and federal level. Those hospitals are further classified as primary, secondary and tertiary health institutions. The covid-19 pandemic has a serious effect on service delivery to patients in Nigeria as it can be noticed in our study which shows that only 88.1% of our respondents claimed that their surgical outpatient departments (SOPD) are rendering services during the period. Some centers have an isolation center to manage covid -19 patients but little percentage of them have a dedicated team to manage covid-19 patients. From this study it was shown that less than half of the respondents had access to PPE as frontline health care/workers. This is contrary to what is obtainable in UK where it was recommended that all staff should have personal protective equipment (PPE) , up-to-date training on COVID-19 and been regularly tested for the virus 11. And only 33.9% had a formal training as to the use of PPE. Operations on elective cases were reduced to 45% during this pandemic. The reasons are not far-fetched as majority of the institutions cannot meet the criteria to keep the universal precautions when it comes to managing patients during this period. Other factors may include the role of anaesthetist. Although unproven in people with COVID-19, preference for regional anaesthetic over general anaesthesia has advantages such as minimal effect on the respiratory system, avoidance of intubation-related seeding of pathogens to the lower respiratory tract, decreasing thromboembolic complications, and a reduced surgical stress response.12, 13 Using regional anaesthetic techniques, aerosol-generating procedures can be avoided with decreased risk to health personnel; additionally, there is potential to conserve protective equipment and essential drugs during shortages. 14. It is important to note that the choice of anaesthetic is determined by the surgical procedure, patient parameters, and a shared decision between the patient and the physician. The level of preparation in some institution was very poor as our respondents claimed that they only recorded 11% satisfactory. The average weekly surgical cases were also reduced from this study.
Limitation
The limitation of this study is that the convenience sampling method has an inability to generalized the results of this survey to the population as a whole.
Conclusion
COVID-19 has led to reduction in surgical outpatients, significant reduction in elective surgeries in Nigeria. Adequate PPE needs to be provided, there should be guidelines for safety for future. There should be adequate preparation should there be any pandemic in the near future.
References
- 1.CDC. (2019) Novel Coronavirus. CDC. Available at https//www.cdc.gov/coronavirus/ 2009-ncov/about/index.html , Wuhan, China .
- 2.Gallegos A. (2020) WHO Declares Public Health Emergency for Novel Coronavirus. Medscape Medical News. Available athttps://www.medscape.com/viewarticle/924596.January 30,2020;.
- 3.Ramzy A, McNeil D G. (2020) WHO Declares Global Emergency as Wuhan Coronavirus Spreads. The New York Times. Available at htt://nyti.ms/2RER70M.
- 4. (2020) The NEW York Times. Coronavirus Live Updates: W.H.O. Declares Pandemic as Number of Infected Countries Grows. The New York Times. Available athttps://www.nytimes.com/2020/03/11/world/coronavirus-news.html#link-682e5b06.
- 5. (2020) Coronavirus Updates: The Illness Now Has a Name: COVID-19. The New York Times. Available athttp://www.nytimes.com/2020/02/11/word/asia/coronavirus-china.html.
- 6. (2020) WHO Director-General’s remarks at the media briefing on 2019-nCoV. Available athttp://www.who.int/dg/speeches/detail/who-director-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020
- 7.Gorbalenya A E. (2020) Severe acute respiratory syndrome-related coronavirus-The species and its viruses, a statement of the Coronavirus Study Group. Available athttps://doi.org/101101/2020.02.07.937862.
- 9.Shoaib M. (2020) Coronavirus disease 2019pandemic: epidemiology, pathogenesis and challenges. , Journal of Medical Case Reports and Reviews 3(3), 636-639.
- 10.Cascella M, Rajinik M, Cuomo A, Dulebohn S C, DiNapoli R. (2020) Features, evaluation and treatment coronavirus (COVID-19).Treasure Island,Fl,: Stat-Pearls.
- 11.Preparing for surgery during the COVID-19 pandemic :https://www.versusarthritis.org/about-arthritis/treatments/surgery/preparing-for-surgery-during-the-covid-19-pandemic/.
- 12.AJR Macfarlane, Harrop-Griffiths W, Pawa A. (2020) Regional anaesthesia and COVID-19: first choice at last?. , Br J Anaesth 125, 243-47.