
Social Network Analysis of Integrated Medical Services for Hypertension – Using District Hospitals of Shanghai as a Model
Abstract
Objective
To examine the current linkage between different medical services for hypertension patients for enhanced integration among medical service systems.
Methods
A total of 18 hospitals and community medical centers from a district of Shanghai were enrolled for social network analysis which covered emergency visits and hospitalization records of 171,177 outpatients with hypertension. Stata software was used for data preprocessing and UCINET software was used for network analysis of medical service providers to quantify and visualize the network tightness and the "main role" of information delivery of the medical institution network in the area.
Results
The service network of hypertension consultation institutions in the region is closely connected as a whole, but the level of diagnosis and treatment of medical services in various communities varies widely, and the degree of association with higher-level medical institutions is not uniform.
Conclusion
Based on the limited tightness of various medical service providers, it is necessary to implement the responsibilities of individual medical institutions at different levels and pay more attention to improving the service capabilities of primary medical institutions for enhanced integrating medical services in future.
Article Information
- Received
- Accepted
- Published
Academic Editor: Sasho Stoleski, Makedonska brigada 43, 1000 Skopje, Macedonia
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2020 Ziyou Chen, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Yuanan Lu, University of Hawaii at Manoa, Honolulu, HI, USA —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Acknowledgements
The authors are grateful to the Shanghai Health Development and Research Center for the support for this study.
Citation:
Introduction
The survey data of Chinese residents' nutrition and health status in 2002 showed that the prevalence of hypertension in adults over 18 years of age in China was 18.8%. The Report on the Status of Nutrition and Chronic Diseases of Chinese Residents (2015) indicated that the prevalence of hypertension in adults over the age of 18 reached 25.2% in 2012, showing an increasing trend of the prevalence of hypertension in China. It is estimated that there are about 270 million people with hypertension in the country. The increasing prevalence of hypertension has caused serious public health problems 1, 2. Therefore, providing timely and continuous medical services to patients with hypertension is one of the key health tasks at the moment 3.
Integration of medical resources is an important part of modern medical service. The international exploration on the integration of medical resources started in the 1990s. And the integration forms mostly complemented their own medical insurance systems, for example, the American set up responsible medical organizations and patient service medical centers, the British established clinical practice alliance, and the German developed hospital group 4, 5, 6. The World Health Organization proposed an integrated approach in 2007 to eliminate broken and fragmented health services 7. With the advocacy of the World Health Organization, integrated medical services have been actively promoted in developed countries such as Europe and the United States, and have become the core concept of health care and long-term care policy reform in developed countries. In response to the serious aging situation, Japan provides community-based composite services, which is supported by systems and laws. The United States emphasizes the human-based approach and promotes integration at different levels within the health system, which encourages the full use of information systems to achieve information sharing and also to help the physician follows the clinical path. Multi-country practice has proven that integrated medical and health services are an effective way to improve medical quality and patient satisfaction 8. China has been working on the development of an integrated medical and health service system, but such development is relatively slow. The integration-oriented measures are mainly reflected in the promotion of the hierarchical diagnosis and treatment system and the construction of medical unions. This notion has encountered many issues, such as uneven distribution of medical resources, shortage of grassroots talents, medical insurance not matching the hierarchical diagnosis and treatment system, and failure to achieve comprehensive and effective information sharing 9, 10, 11. In general, the direction for the development of China's integrated medical services is not well focused and in-depth. However, in some areas such as Shanghai and Guiyang, it started to explore a family doctor accountability system basing on local economic conditions and actual needs.
To address the present problem of the broken connection between medical institutions at various levels in the medical service network system and between departments within medical institutions, the UCINET social network analysis was performed basing on health big data and medical treatment big data of a district in Shanghai by taking common chronic disease-hypertension as target disease. NetDraw software was used to draw a visual network diagram to present the advantages and limitations of the association status of hypertension integrated medical services in a district of Shanghai.
Material and Methods
Data Information
The data information comes from the big data of a health network in a district of Shanghai, including the health records data and diagnosis and treatment records of the residents in the archives. Each patient visits once and displays a record in the health big data. There were 1,695,903 original records of patient visits in the information of outpatient emergency records and hospitalization records, and a total of 171, 177 patients with hypertension were involved.
Basic information of the medical patients was obtained from the big data on health files through multiple indicators, including the ID number, gender, age, visiting medical institution code, appointment date, medical record (illness), and total cost. Referral record of each hypertension patient was compiled basing on each visit of the same patient. Then network analysis matrix was generated according to the patient referral record.
Basic Information of the Data
Analysis of the basic data of the survey respondents found that the proportion of male and female patients with hypertension is very close, and the age distribution of the population is mainly concentrated between 46 and 85 years old. Table 1 shows the basic information of patients with hypertension in the district of Shanghai in 2017. The medical institutions in Shanghai are roughly divided into three levels: tertiary hospitals, secondary hospitals, and basic community health service centers. Because tertiary hospitals are presently in the early stages of construction and there is not enough data for research and analysis. Thus, big data does not include records of patient visits to new tertiary hospitals. The total cost of hypertension visits the 18 medical institutions covered in the data records is about 281 million. Among these medical services, community health service center has the highest proportion of total expenses for hypertension visits, and secondary hospitals in the district (including hospital D, hospital F, hospital C, hospital A, hospital E, and hospital B) account for a relatively small proportion. The detailed proportion of the total cost of hypertension in each hospital in Shanghai in 2017 is summarized in Table 2.
Table 1. Basic information of patients with hypertension in a district of Shanghai in 2017| Basic index | N (participants) | Composition ratio (%) |
|---|---|---|
| Total | 171177 | 100.00 |
| Male | 83768 | 48.94 |
| Female | 87409 | 51.06 |
| Age | ||
| ≤ 45 | 10423 | 6.10 |
| 46-55 | 23301 | 13.60 |
| 56-65 | 52414 | 30.60 |
| 66-75 | 47996 | 28.00 |
| 76-85 | 27328 | 16.00 |
| 86-95 | 9333 | 5.50 |
| ≥96 | 382 | 0.20 |
| Order | Medical institution | Total cost (yuan) | Proportion of total cost (%) | Rank |
|---|---|---|---|---|
| 1 | A (Hospital) | 5976600 | 2.13 | 16 |
| 2 | B (Hospital) | 21800 | 0.01 | 18 |
| 3 | C (Hospital) | 8054600 | 2.87 | 15 |
| 4 | D (Hospital) | 18000000 | 6.41 | 8 |
| 5 | E (Hospital) | 3671600 | 1.31 | 17 |
| 6 | F (Hospital) | 22600000 | 8.05 | 3 |
| 7 | G (CMSC*) | 17200000 | 6.13 | 9 |
| 8 | H (CMSC) | 22471300 | 8.01 | 4 |
| 9 | I (CMSC) | 24003600 | 8.55 | 2 |
| 10 | J (CMSC) | 22300000 | 7.95 | 5 |
| 11 | K (CMSC) | 21200000 | 7.56 | 6 |
| 12 | L (CMSC) | 19300000 | 6.88 | 7 |
| 13 | M (CMSC) | 11608300 | 4.14 | 11 |
| 14 | N (CMSC) | 8486500 | 3.02 | 14 |
| 15 | O (CMSC) | 40300000 | 14.36 | 1 |
| 16 | P (CMSC) | 10900000 | 3.89 | 12 |
| 17 | Q (CMSC) | 10500000 | 3.74 | 13 |
| 18 | R (CMSC) | 14000000 | 4.99 | 10 |
| — | Total | 280594300 | 100 | — |
Patient Referral Flow Information
Every visiting record of hypertension patient was collected from the big data of residents' health files in the district of Shanghai. The analysis of referral flow data of hypertension patients covered the outpatient record, the emergency record, and the inpatient record. The referral data information of hypertension patients was compiled according to the ID number of the patient with hypertension, the code of the visiting medical institution, and the date of the patient's referral and medical treatment. Patient referral data sheets in the form of "institution-institution" was generated and further processed by using statistical software Stata / SE 15.1. These together allowed to obtain the patient turnover in different institutions in the district of Shanghai in 2017, which was used as the basic data matrix for social network analysis (Table 3).
Table 3. Matrix of admission of medical institutions in a district of Shanghai in 2017| A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | |
| A | 0 | 0 | 14 | 60 | 0 | 56 | 4713 | 14 | 162 | 15 | 540 | 12 | 1 | 5 | 40 | 16 | 6 | 18 |
| B | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 0 |
| C | 14 | 0 | 0 | 134 | 0 | 51 | 16 | 9 | 12 | 14 | 74 | 121 | 2 | 1 | 6458 | 12 | 9 | 12 |
| D | 63 | 4 | 140 | 0 | 2 | 1240 | 83 | 2575 | 1437 | 3425 | 48 | 1197 | 1246 | 780 | 1028 | 8 | 1591 | 1811 |
| E | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 |
| F | 53 | 1 | 58 | 1258 | 1 | 0 | 83 | 1402 | 1516 | 3168 | 110 | 457 | 1336 | 835 | 468 | 7 | 1457 | 1947 |
| G | 3478 | 0 | 16 | 71 | 0 | 77 | 0 | 24 | 290 | 78 | 293 | 14 | 7 | 4 | 79 | 66 | 17 | 65 |
| H | 13 | 2 | 3 | 2255 | 2 | 1222 | 22 | 0 | 335 | 1937 | 8 | 214 | 64 | 159 | 81 | 3 | 747 | 535 |
| I | 139 | 0 | 10 | 1206 | 1 | 1329 | 277 | 237 | 0 | 420 | 28 | 40 | 39 | 12 | 110 | 34 | 127 | 2282 |
| J | 9 | 0 | 11 | 2988 | 1 | 2784 | 87 | 2177 | 495 | 0 | 15 | 307 | 194 | 216 | 243 | 2 | 2204 | 1855 |
| K | 447 | 0 | 59 | 35 | 0 | 77 | 289 | 9 | 25 | 15 | 0 | 17 | 0 | 2 | 245 | 724 | 18 | 9 |
| L | 10 | 1 | 104 | 1116 | 0 | 438 | 14 | 252 | 53 | 346 | 18 | 0 | 6 | 17 | 223 | 4 | 166 | 119 |
| M | 2 | 0 | 1 | 1089 | 0 | 1220 | 7 | 78 | 37 | 217 | 0 | 7 | 0 | 157 | 8 | 0 | 469 | 399 |
| N | 2 | 0 | 2 | 768 | 0 | 830 | 5 | 168 | 19 | 237 | 3 | 16 | 164 | 0 | 9 | 1 | 258 | 285 |
| O | 36 | 1 | 5701 | 967 | 0 | 462 | 81 | 112 | 134 | 263 | 261 | 208 | 6 | 9 | 0 | 67 | 102 | 104 |
| P | 8 | 0 | 7 | 4 | 0 | 6 | 62 | 6 | 39 | 7 | 759 | 6 | 0 | 0 | 71 | 0 | 3 | 13 |
| Q | 3 | 0 | 5 | 1348 | 0 | 1241 | 19 | 662 | 130 | 2193 | 13 | 125 | 459 | 223 | 84 | 3 | 0 | 632 |
| R | 15 | 1 | 12 | 1747 | 9 | 1896 | 82 | 688 | 2774 | 2178 | 5 | 119 | 487 | 264 | 110 | 18 | 758 | 0 |
Social Network Analysis
Based on big data, the social network analysis was mainly conducted to empirically analyze the situation of integrated medical services for hypertension in a district of Shanghai. Social network analysis is formed by the cross-disciplinary combination of social science and mathematics, statistics, and computing methodology. It can be used to change some abstract relationship problems to be quantitative, and presents the problems with clear and easy-to-understand visualization diagrams 12. The social network diagram is mainly composed of points and lines. The points represent members or actors in the network, and the lines connecting the points represent the relationship between two actors. This relationship is based on the establishment of information transfer and sharing. Social network analysis covers relationship, network, and structure three main concepts.
Relationship refers to the connection between members in the network or the association based on an event, and is generally considered to be closely related to the flow and sharing of information 13, 14. The network is determined based on the boundary of the research purpose and is composed of one or more actors and one or more relationships among them 15. The network structure is mainly analyzed by measures such as point centrality and centralization of the graph. Thereby presenting the structural characteristics of the network 16.
In order to analyze the connection, cohesion, contribution and status of medical institutions in the service network of medical institutions in the region, five indexes of point centrality, eigenvector centrality, betweenness centrality, k-core analysis and network density were selected.
Point centrality is used to measure the direct impact of network members, because patients’ medical choices can reflect the active level of the medical institution. The importance of an actor is related to the connected actors’ importance in the network. By measuring the eigenvector centrality, the core actors in the network are determined. Betweenness centrality is assessed to identify the "middleman" of information dissemination. In the calculation of k-kore index, the network cohesion is analyzed by assigning k multiple times to divide the network into different cohesive groups. Through the network density measurement, the association degree of actors in the entire network is analyzed. The higher the density value, the higher the relevance of actors in the network and the more complete the social network graph. In an ideal social network diagram, a density value of 1 indicates that members of the network are related to other members.
Results
This article reveals the flow of patients with hypertension in medical institutions in the district of Shanghai, the degree of association between the institutions in the hypertension service network, the contribution of each medical institution in the network, and the degree of cohesion of member institutions in the network. These data were analyzed and calculated according to 5 social network analysis indicator systems including point centrality, eigenvector centrality, betweenness centrality, k-core, and network density, and analysis results was visualized by generating a social network diagram.
Point Centrality Analysis
In the network of hypertension medical institutions in the case area, each point represents a medical institution in the network 17. Based on the principle of point centrality, the number of hypertensive patients transferred in and out of each medical institution was determined to quantify the information control capabilities of each medical institution.
As shown in Table 4, Hospital D is the medical institution with the highest number of transferred-in and out of hypertension patients, indicating that Hospital D is closer to other members of the network and has a higher degree of tightness. Thus, this hospital is likely to be at the core and have an impact on the actions of other members of the network. Among the 18 medical institutions in the district, there are 5 secondary hospitals and 13 community health service centers. Among the top 5 medical institutions with a large number of patients transferred out and transferred, Secondary hospitals account for 40% (Hospital D and Hospital F) while community health service centers account for 60%. Further analysis shows that, 10 of the 18 medical service providers showed an indegree value greater than the outdegree value, that is, the number of patients transferred in was more than the number of patients transferred out.
Table 4. Circulation of hypertension patients in various medical institutions in a district of Shanghai in 2017| Medical institution | Outdegree | Indegree |
|---|---|---|
| D (Hospital) | 16678 | 15048 |
| F (Hospital) | 14157 | 12930 |
| J (CMSC)* | 13588 | 14515 |
| R (CMSC) | 11163 | 10088 |
| O (CMSC) | 8514 | 9258 |
| H (CMSC) | 7602 | 8413 |
| Q (CMSC) | 7140 | 7933 |
| C (Hospital) | 6939 | 6143 |
| I (CMSC) | 6291 | 7458 |
| A (Hospital) | 5672 | 4292 |
| G (CMSC) | 4579 | 5840 |
| M (CMSC) | 3691 | 4011 |
| L (CMSC) | 2887 | 2861 |
| N (CMSC) | 2767 | 2684 |
| K (CMSC) | 1971 | 2175 |
| P (CMSC) | 991 | 965 |
| E (Hospital) | 5 | 16 |
| B (Hospital) | 5 | 10 |
(Figure 1) shows that most medical institutions present the characteristics that more numbers of patients are transferred in than transferred out. The number of hypertensive patients admitted by the top five medical and health service institutions accounted for 53.95% of the total number of consultations, which includes 24.41% in secondary hospitals and 29.54% in three community health service centers. This result reveals the importance of community health service centers in the diagnosis and treatment of hypertension in the district.
Figure 1. Comparison of out-degree and in-degree of each medical institution. The Horizontal axis is the medical institution and the vertical axis is the degree value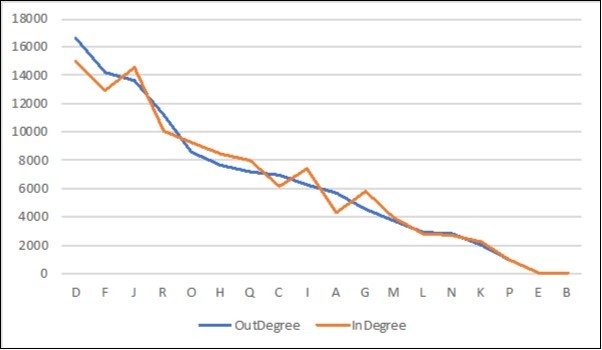
Download figure
Eigenvector Centrality Analysis
The influence of members in the network is not only related to the number of members related to it, but also shows the importance of the members themselves connected to the network. The higher the importance of the associated members themselves, the higher their eigenvector values 16. By measuring the centrality of the feature vector, the core members of the medical institution service network were identified. As shown in Table 5, the four medical institutions of hospitals D and F, and community centers H and R have the same and highest measured values. It can be determined that these four medical institutions are relatively more important in network association than other members. In a network, a member is associated with more important members, the more likely that this member is to occupy a more important position in the network, Therefore, these four medical institutions will play a certain important role in the network. Whereas, the lower calculation results presented by Hospitals B and E could reflect their relatively low degree of correlation with important members in the network. In other words, members associated with hospitals E and B are insignificant in the network.
Table 5. Measurement results of eigenvector values of 18 medical institutions| Medical institution | Eigenvector | nEigenvector |
|---|---|---|
| F (Hospital) | 0.258 | 36.514 |
| D (Hospital) | 0.258 | 36.514 |
| R (CMSC) | 0.258 | 36.514 |
| H (CMSC) | 0.258 | 36.514 |
| L (CMSC) | 0.252 | 35.626 |
| Q (CMSC) | 0.252 | 35.626 |
| O (CMSC) | 0.252 | 35.626 |
| I (CMSC) | 0.251 | 35.479 |
| J (CMSC) | 0.251 | 35.479 |
| G (CMSC) | 0.245 | 34.59 |
| A (Hospital) | 0.245 | 34.59 |
| N (CMSC) | 0.245 | 34.59 |
| C (Hospital) | 0.245 | 34.59 |
| P (CMSC) | 0.231 | 32.698 |
| K (CMSC) | 0.231 | 32.698 |
| M (CMSC) | 0.216 | 30.538 |
| B (Hospital) | 0.118 | 16.71 |
| E (Hospital) | 0.101 | 14.337 |
Betweenness Centrality Analysis
If two non-adjacent actors in the network want to make contact, they must pass through other actors in the network, and these "other actors" are generally on the path between the two actors. Thus, "other actors" could control the information transmission and other possible an actor is on the geodesic distance of many actor pairs, it means that the actor has a high betweenness centrality 17. In a medical service provider network, when an actor has a high degree of betweenness centralism, it means that the actor has a greater degree of influence on the patient's choice of referral and medical treatment, and it will also affect the association between medical institutions. Table 6 shows the measured betweenness centrality values of various institutions in the network of hypertension consultation medical institutions in the district of Shanghai. The betweenness of actors in the network is even more clearly presented by a visualization diagram of the betweenness centrality based on the measured betweenness centrality (Figure 2). The size of the point in Figure 2 is directly related to the value of the median centrality value of the point. The arrow pointing indicates the direction of turning in and out. As shown in Table 6, communities R and H, and hospitals D and F have the largest measured betweenness centrality. Therefore, among the 18 medical institutions in the network referred by hypertension patients, these four hospitals occupy an important position for information sharing on the network. Most members of the network will more likely to concentrate on these four medical services. These four hospitals have largely controlled the connection with other members of the network in the medical treatment of hypertension. In contrast, the five medical service agencies with a betweenness centrality value of 0are on the edge of the network, and have weak connections with other members in the network with the least impact on the activities of other members.
Figure 2. Betweenness Centrality. The red squares in the figure represent hospitals, and the blues represent the community health service centers. The size of the squares is proportional to the betweenness centrality value. The higher the centrality value, the larger the square. The thicker the lines, the closer the connection.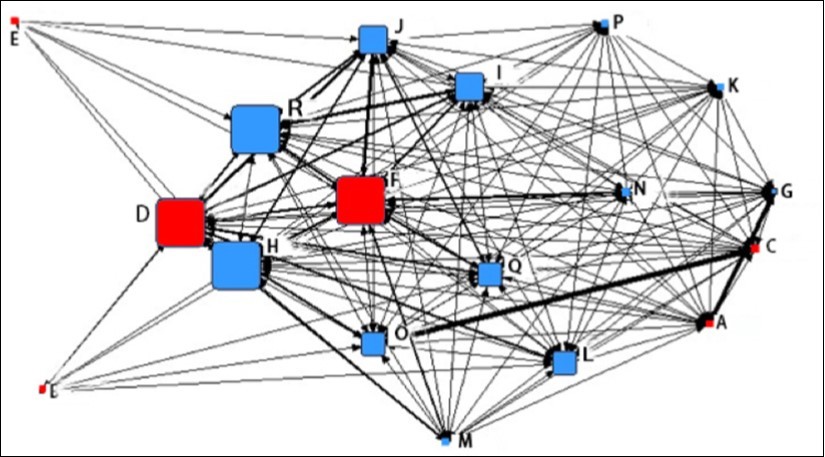
Download figure
| Medical institution | Betweenness | nBetweenness |
|---|---|---|
| R (CMSC) | 3.356 | 2.468 |
| H (CMSC) | 3.356 | 2.468 |
| D (Hospital) | 3.356 | 2.468 |
| F (Hospital) | 3.356 | 2.468 |
| I (CMSC) | 1.821 | 1.339 |
| J (CMSC) | 1.821 | 1.339 |
| L (CMSC) | 1.440 | 1.059 |
| O (CMSC) | 1.440 | 1.059 |
| Q (CMSC) | 1.440 | 1.059 |
| G (CMSC) | 0.154 | 0.113 |
| A (Hospital) | 0.154 | 0.113 |
| C (Hospital) | 0.154 | 0.113 |
| N (CMSC) | 0.154 | 0.113 |
| B (Hospital) | 0.000 | 0.000 |
| E (Hospital) | 0.000 | 0.000 |
| M (CMSC) | 0.000 | 0.000 |
| K (CMSC) | 0.000 | 0.000 |
| P (CMSC) | 0.000 | 0.000 |
K-core Analysis
Through observing the distribution of agglomerate subgroups, agglomerate subgroups in the provider-provider network can be identified. These findings would allow to further analyzes what outstanding characteristics a specific medical institution has with a certain medical institution as its core. The k-core analysis results of 18 medical institutions in the network are shown in Figure 3, a more visualized diagram for the results.
Figure 3. K-core analysis results. One shape in the figure represents one partition, and four shapes of diamond, square, circle, and triangle represent four partitions.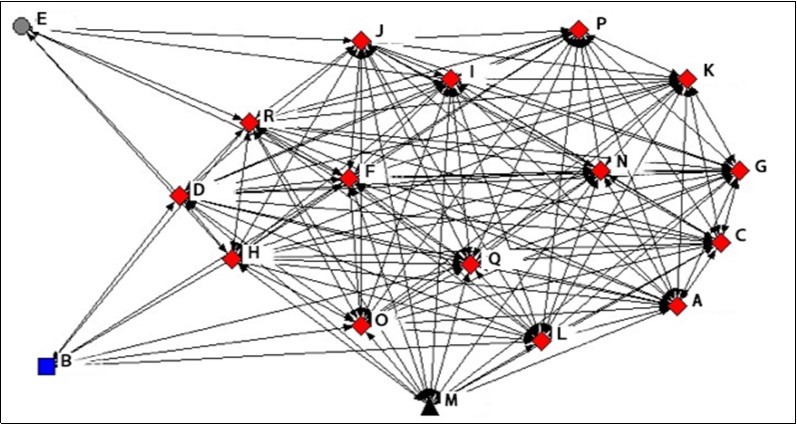
Download figure
Among the 18 medical institutions, they can be divided into 4 groups according to their degree scores: 6, 7, 13, and 14. The groups 6 (6-Core), 7 (7-Core), 13 (13-Core), and 14 (14-Core) included all 18 (all), 17, 16, and 15 medical institutions in the network, respectively. 14-Core contains 15 medical institutions including 1,3,4,6,7,8,9,10,11, 12,14,15,16,17,18, which means any two among these 15 medical institutions are linked.
As shown in Figure 3, the four shapes of diamond, square, circle, and triangle represent four different partitions. The diamond-marked partitions correspond to the 15 specific medical institutions with a "Degree" value of "14", which have the closest relationship. Hospitals E (round), hospital B (square), and community center M (triangle) are located at the edge of the network. Among them, hospital E has the least number of associated members in the network, followed by Hospital B. This means these two medical institutions are at the outermost edge of the network and have the least contact with other medical institutions in the district.
Network Density Analysis
Considering the closeness of the connections between the nodes as a whole, we can understand the sparseness of the relationship between service providers by calculating the tightness of the medical institutions network. In the analysis of the overall network, the specific directional relationship between network members is temporarily abandoned. As long as there is a transfer-in or transfer-out relationship between two points, the two actors are considered to be connected 17. The calculation formula is C=1-[ ] (V=22,N=18). Therefore, the measured value of the overall network density is 0.856, which is close to 1, which indicates that members in the network are more closely connected, the speed and efficiency of information flow between members is relatively high, and the information channel is relatively smooth.
] (V=22,N=18). Therefore, the measured value of the overall network density is 0.856, which is close to 1, which indicates that members in the network are more closely connected, the speed and efficiency of information flow between members is relatively high, and the information channel is relatively smooth.
Discussion
This study revealed that the hypertension medical service network in the district shows a relatively close relationship overall. The measured value of the overall network density is high (0.856), which shows that the medical institutions in the network are closely connected. Thus, the speed and efficiency of information circulation between the institutions are high, and the information circulation channel is smooth. This area can further improve the residents' health data information system and effectively promote the integration of medical and health services based on existing advantages. In this way, the health and diagnostic information of residents can be fully shared among different medical institutions, and repeated consultations can be avoided, thereby reducing patient medical costs and waste of health resources.
This study also revealed that the secondary hospital D in the district is the center of the integrated medical service network for hypertension. The analysis results of the direct and indirect links between medical institutions indicate that the hospital D with the highest central value of the degree and the central value of the feature vector is more closely linked to other members of the network. Analysis of the results indicates that the role of the "prevention and treatment center" of hypertension in the region is mainly assumed by the secondary hospital and hospital D and its related to other medical institutions. Regional secondary hospitals have a relatively high level of diagnosis and treatment of hypertension, play a leading role in regional hypertension integrated services, and have formed better cooperative relationships with medical institutions at lower levels in the network. Analysis results of the integrated service network of hypertension in the district are consistent with the functions of the regional secondary hospitals. In order to improve the efficiency of cooperation between medical institutions, it is important to focus on standardizing the cooperation mechanism between medical institutions, and clearly and effectively implementing the division of responsibilities of medical institutions at all levels.
A few community health service centers in the district also play a relatively important rule in the integrated medical service for hypertension. However, the level of diagnosis and treatment of medical and health service institutions in various communities is not same. Among the secondary and tertiary hospitals, community health service centers and clinics in the region, five medical institutions are the main contributors in the hypertension medical service network, including two secondary hospitals and followed by three community health service centers. These findings indicate that the regional community health service centers play a relatively important rule in the prevention and treatment of hypertension in the region. These results are consistent with the fact that the total cost of community health service centers ranks high in the basic information analysis, and is consistent with the implementation of patient-centered integrated medical service initiatives centered at primary medical institutions. However, the resource utilization efficiency in some primary medical institutions needs to be further improved. This may be done by exploring the medical community or medical consortium pilots in combination with its own actual situation, and striving to improve the capacity of primary health care services in order to improve the important position of community health service centers in the prevention and treatment of hypertension.
This analysis demonstrated that most medical institutions shared a same pattern of patient transfer: more transfer-in patients than transfer-out ones. One of main driving force for this easy to transfer in but difficult to transfer out is the interest of medical institutions at all levels 18. Another factor for easy to transfer in is due to the lack of uniform implementation standard for transfers, and referrals are mostly based on internal criteria of each medical unit. Thus, it is important to establish specific consultation and referral standards and standardize referral principles. Medical service centers at all levels, in combination with integration requirements and patient specific conditions, formulate referral rules to coordinate the referral cooperation of hospitals at all levels. This will allow to better utilize the functional advantages of hospitals at all levels, and make better use of medical and health resources. At the same time, more attention needs to be paid to the introduction of talents, such as to invite expert to community medical service centers for consultation and guidance through cooperation with tertiary hospitals. With the constant improvement of the service capabilities of primary medical institutions are constantly improving, more patients in need will be attracted to seek treatment at the grassroots level, thereby achieving the purpose of the first consultation at the grassroots level.
Conclusion
This study showed that the closeness of contact between different medical institutions varies greatly, which could be due to limited service capabilities of primary medical institutions, less effective management of governmental departments on balancing the interests of related parties when making overall plans, and incomplete coverage of health information data platforms. Therefore, comprehensive medical service integration requires strengthening the service capacity building of primary medical institutions and building a health information data platform covering the entire population. The government health management department should pay attention to balancing the interests of multiple parties and continuously strengthen overall planning and supervision and management.
Affiliation
ZYC: data collation and analysis, manuscript preparation
JSL: study design, manuscript planning and revision
FL: data collation and analysis, manuscript preparation
YL: Data and manuscript preparation and revision
References
- 1.Arrey W, Dimala C, Atashili J, Mbuagbaw J, Monekosso G. (2016) an. Emerging Problem in Rural Cameroon: Prevalence, Risk Factors, and Control. , International Journal of Hypertension 6.
- 2.He H, Pa L, Pan L, Simayi A, Mu H et al. (2018) of BMI and Its. Optimal Cut-Off Value in Identifying Hypertension in Uyghur and Han Chinese: A Biethnic Study from the China National Health Survey (CNHS). , International Journal of Hypertension 8.
- 3.Doumas M, Papademetriou V, Douma S, Faselis C, Tsioufis K et al. (2011) . Benefits from Treatment and Control of Patients with Resistant Hypertension.International Journal of Hypertension 8.
- 4.Lewis S, Damarell R A, Tieman J J, Trenerry C. (2018) Finding the Integrated Care Evidence Base in PubMed and Beyond: A Bibliometric Study of the Challenges.International Journal of Integrated Care. 18(3), 11.
- 5.MNM Mirella. (2011) A development model for integrated care.International. , Journal of Integrated Care 11(7), 099.
- 6.Whelton P K, Carey R M, Aronow W S. (2018) 2017ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention,detection ,evaluation,and management of high blood pressure in adults:a report of the american college of cardiology/american heart asso - ciation task force on clinical practice guidelines.J Am CollCardiol. 71(19), 2273-2275.
- 8.Busetto L, Luijkx K, Calciolari S, LGG Ortiz, HJM Vrijhoef. (2018) . Barriers and Facilitators to Workforce Changes in Integrated Care.InternationalJournal of Integrated Care.18(2): 17.
- 9.Gao Y, Haoling Gong HL, Wang Q, Wang H, Zhuang L M. (2019) . Practice of Nursing Service Improvement in Establishing Medical Union Health Service System.Chinese Nursing Research 33(06), 1080-1083.
- 10.1Pan Y, Liu H Y, Sun H T. (2018) Exploration and reflection on the cooperation model of the cross-regional medical consortium in our hospital.Chinese Hospital management. 38(08), 57-59.
- 11.Zheng D X, Liang Y P, Feng X. (2018) Definition of connotation and extension of medical complex.Chinese Hospital management. 38(08), 1-3.
- 12.Otte E, Rousseau R. (2002) Social network analysis: a powerful strategy, also for the information sciences.Journal of Information Science. 28(6), 441-453.
- 13.Bower C, Fridkin D, Wolford H. (2020) Evaluating movement of patients with carbapenem-resistant enterobacteriaceae infections in the greater atlanta metropolitan area using social network analysis.Clinical InfectiousDiseases. 70(1), 75-81.
- 14.Steitz B D, Levy M A. (2016) A Social Network Analysis. of Cancer Provider Collaboration.AMIA Annual Symposium proceedings Archive 1987-1996.
- 15.Holtrop J, Ruland S, Diaz S, Morrato E, Jones E. (2018) Using Social Network Analysis to. Examine the Effect of Care Management Structure on Chronic Disease Management Communication Within Primary Care.Journal of General Internal Medicine.33(5): 612-620.