
Duodenocolic Fistula: A Rare Complication of Gastrointestinal Tuberculosis
Abstract
Introduction
Case
This is a case of a 28-year-old Filipino female who presented with periumbilical pain for five months, with associated anorexia, fever, and weight loss. Biopsy showed chronic granulomatous inflammation with caseation necrosis and Langhan’s type giant cells consistent with tuberculous etiology (Figure 6 and Figure 7). Category I Anti-TB treatment for six months was started and the service planned to repeat both colonoscopy and CT-scan after the initial round of anti-TB treatment.
Conclusion
Benign duodenocolic fistula in the form of extrapulmonary TB is a rare GI finding that is triggered by inflammatory processes. Proper management in this case was to treat the underlying TB infection which is endemic in the Philippines.
Article Information
- Received
- Accepted
- Published
Academic Editor: Carlo Aprile, IRCCS Fond. Policlinico San Matteo - Pavia-Italy.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2022 Julian Iñaki L. Garcia, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Julian Iñaki L. Garcia, Department of Gastroenterology, De La Salle University Medical Center —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Duodenocolic fistula secondary to tuberculosis is a rare entity. There is a myriad of etiologies for fistula formation, among those reported include malignancy, previous abdominal surgery, inflammatory bowel disease (IBD), cystic fibrosis, and tuberculosis (TB) 1.
A benign duodenocolic fistula is also known as a tract between the duodenum and colon or the cecum with non-malignant origin. These fistulas are less common than malignant fistulas and may be secondary to peptic ulcer disease (PUD), biliary tract disease, ulcerative colitis, regional enteritis, appendicitis, caseating tuberculous lymph nodes, or perforating duodenal diverticula 2,3. In the Philippines, TB is endemic and there are a small number of cases that involve extrapulmonary TB, including gastrointestinal (GI) TB. This report presents a rare case of a duodenocolic fistula, which to the extent of the authors' knowledge, is the first case reported in the region.
Case Report
This is a case of a 28-year-old Filipino female who presented with periumbilical pain for five months, with associated anorexia, fever, and weight loss in the subsequent days. Three days prior to admission, patient noted an onset of hematochezia and hematemesis. Examination of the abdomen noted hyperactive bowel sounds and tender periumbilical and right lower quadrant pain, and no organomegaly was noted.
Esophagogastroduodenoscopy (EGD) revealed a fistulous opening in the third part of the duodenum and a bleeding vessel. (Figure 1) Bleeding was controlled with injection hemostasis and 3 hemoclips were deployed. The colonoscopy revealed a large obstructing, polypoid, ulcerating, and circumferential mass with areas of necrosis that was seen at the proximal transverse colon which precluded further advancement of the scope. Biopsy samples were sent for histopathology investigation and TB polymerase chain reaction (PCR) test.
Figure 1. EGD findings of a pathologic lumen and a bleeding vessel were seen at the third portion of the duodenum.
Download figure
There was no evidence of malignancy or IBD seen during both endoscopic procedures. Computed tomography (CT) scan of the whole abdomen was done which showed inflammatory changes involving the cecum and adjacent duodenum and ileum with coloenteric fistulae. There was noted progression of abdominal lymphadenopathies as well as ascites. Main consideration was an infectious disease process (i.e. TB) (Figure 2, Figure 3, Figure 4 to Figure 5).
Figure 2. Colonoscopy finding of a circumferential, obstructive and nodular mass with areas of necrosis with a pathologic lumen believed to be communicating with the lumen seen on the previous EGD was seen at the proximal transverse which precluded further advancement of the scope 
Download figure
Figure 3. Coronal and axial view of the abdomen, the blue arrows pointing towards the suggestive communication to the ileum.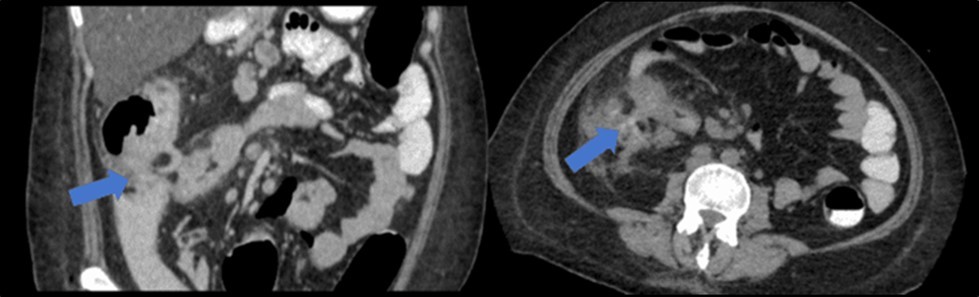
Download figure
Figure 4. Coronal and axial view of the abdomen, the blue arrows pointing towards the suggestive communication to the duodenum 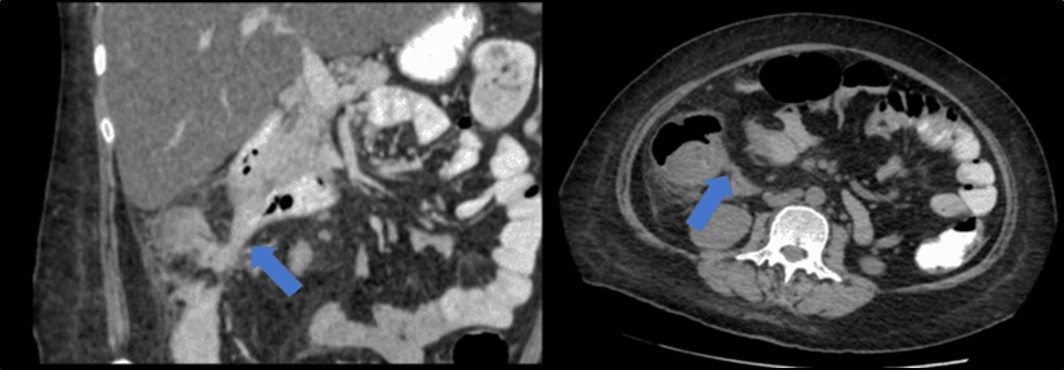
Download figure
Figure 5. Enlarged and necrotic abdominal nodes in the mesenteric, pericecal, pericolic, para-aortic, paracaval and inter-aortocaval regions. Prominent and enlarged nodes also located in the common hepatic and periportal regions
Download figure
Biopsy showed chronic granulomatous inflammation with caseation necrosis and Langhan’s type giant cells consistent with tuberculous etiology (Figure 6, and Figure 7). TB PCR detected Mycobacterium tuberculosis, Rifampicin (MTB, RIF) resistance indeterminate. Category I Anti-TB treatment for six months was started and the service planned to repeat both colonoscopy and CT-scan after the initial round of anti-TB treatment. Currently, the patient is able to work with no abdominal pain and was able to tolerate her anti-TB drug regimen
Figure 6. Pathologic slide in the low power field. The area inside the yellow circle is the area of central necrosis. The portion inside the red circle is the peripheral lymphocytic ring, and inside the green circle is the Langhan’s type multinucleated giant cells 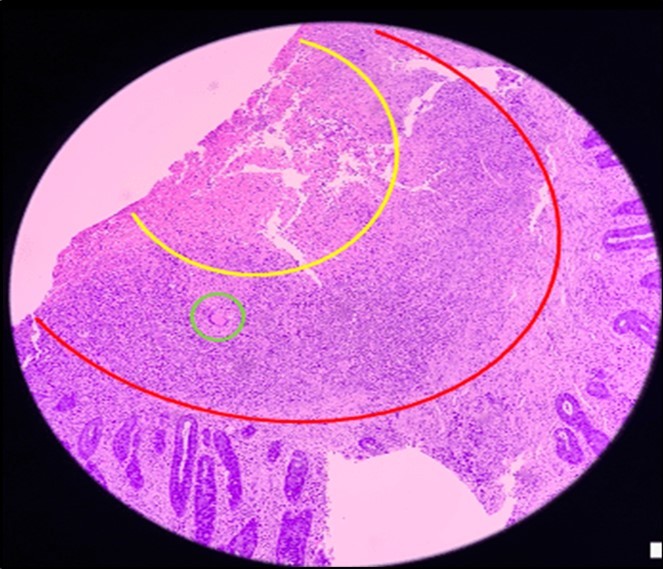
Download figure
Figure 7. Pathologic slide in the high power field. Inside the green circle is the epitheloid histiocytes. The yellow circles are the Langhan’s type multinucleated gian cells. And inside the red circle is the lymphocytic infiltrates. Which is suggestive of tuberculous etiology. 
Download figure
Discussion
Benign duodenocolic fistula is a complication that occurs through a perforation between the duodenum and the mid-transverse column, due to the presence of a duodenal diverticulum 3. This condition is often due to inflammatory diseases of the gastrointestinal tract such as gallstone disease. Crohn’s disease, and even Tuberculosis 4. In some studies, duodenocolic fistulas have been noted as a type of inflammatory response to colon cancer, duodenal cancer, and peptic ulcer disease, among others 1, 4.
Benign duodenocolic fistulas feature colicky abdominal pain, diarrhea, nausea and vomiting as common non-specific symptoms 2,3, 4 The diagnosis of this condition can include upper gastrointestinal barium studies or a barium enema; however, endoscopic evaluation is necessary in proper diagnosis as allows better visualization of the mass, as well as the areas adjacent to it 2, 4. Surgery is the only treatment that could be called a cure for this condition, and En-bloc resection of the tumor-fistula complex is the definitive management of duodenocolic fistulas 3. For those with advanced lesions, palliative care may be the best solution 3.
Tuberculosis-associated duodenocolic fistula is an extremely rare finding among the general population. This case is the first reported for this region of the Philippines. In Gan et al, 2021, it was found that a patient’s previous history of pulmonary tuberculosis was the culprit behind their own illness 1. Abdominal TB may occur as diffuse, white to yellowish peritoneal nodules and ascitic adenosine deaminase (ADA) highly sensitive to TB 1. In countries where TB is endemic, patients are usually started on anti-TB medication as soon as possible. The initiation and continuation of anti-TB medications should be done, and these remain the “cornerstone” of TB treatment even in extrapulmonary cases such as this one1, 3.
Conclusion
Benign duodenocolic fistula in the form of extrapulmonary TB is a rare GI finding that is triggered by inflammatory processes. Proper management in this case was to treat the underlying TB infection which is endemic in the Philippines.
References
- 1.DEY Gan, Sibin R, Payus A O, Hayati F. (2021) Colo-appendico-duodenal fistula: Rare presentation of extrapulmonary tuberculosis. Clin Case Rep. 9(10), 04797.
- 2.Soheili M, Honarmand S, Soleimani H, Elyasi A. (2015) Benign Duodenocolic Fistula: a Case Report. Acta Med Iran. 53(8), 512-5.