
The Follicular Benignancy- Desmoplastic Trichoepithelioma
Abstract
Trichoepithelioma is a benign, cutaneous neoplasm originating from the hair follicle and is categorized into singular trichoepithelioma, multiple trichoepithelioma and desmoplastic trichoepithelioma wherein desmoplastic trichoepithelioma is cogitated as an exceptional, cutaneous adnexal tumour. Desmoplastic trichoepithelioma was initially scripted by Hartzell in 1904 wherein the lesion was described as a benign, cystic epithelioma. Desmoplastic trichoepithelioma can be additionally nomenclated as epithelioma adenoides cysticum, morphea - like epithelioma or sclerosing epithelial hamartoma 1. Familial instances of desmoplastic trichoepithelioma are infrequent and can be misdiagnosed on account of adjunctive benign, cutaneous, adnexal neoplasms depicting subtle clinical features, excepting a nodular basal cell carcinoma. Cogent clinical and histological features can assist the diagnosis of desmoplastic trichoepithelioma 1, 2.
Article Information
- Received
- Accepted
- Published
Academic Editor: Pietro Scicchitano, Cardiology Department, Hospital of Ostuni (BR) - Italy.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Anubha Bajaj
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Corresponding author: Anubha Bajaj, MD (Pathology), Panjab University; Department of Histopathology, A.B. Diagnostics, A-1, Ring Road, Rajouri Garden, New Delhi 110027, India —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Preface
Trichoepithelioma is a benign, cutaneous neoplasm originating from the hair follicle and is categorized into singular trichoepithelioma, multiple trichoepithelioma and desmoplastic trichoepithelioma wherein desmoplastic trichoepithelioma is cogitated as an exceptional, cutaneous adnexal tumour. Desmoplastic trichoepithelioma was initially scripted by Hartzell in 1904 wherein the lesion was described as a benign, cystic epithelioma. Desmoplastic trichoepithelioma can be additionally nomenclated as epithelioma adenoides cysticum, morphea - like epithelioma or sclerosing epithelial hamartoma 1.
Familial instances of desmoplastic trichoepithelioma are infrequent and can be misdiagnosed on account of adjunctive benign, cutaneous, adnexal neoplasms depicting subtle clinical features, excepting a nodular basal cell carcinoma. Cogent clinical and histological features can assist the diagnosis of desmoplastic trichoepithelioma 1, 2.
Disease Characteristics
Desmoplastic trichoepithelioma is an exceptional, benign adnexal tumefaction arising from basal cells of outer root sheath of the hair follicles. With an estimated incidence of 1 : 5000, desmoplastic trichoepithelioma commonly appears in young and middle aged women, demonstrates a female preponderance and usually appears within 8 years to 81 years 1, 2.
Multiple foci of preliminary lesions of desmoplastic trichoepithelioma can concur with foci of basal cell carcinoma, thus indicating a concomitant genetic predisposition. As a tumefaction delineating an autosomal dominant mode of disease inheritance, desmoplastic trichoepithelioma can be associated with basal cell carcinoma or a cylindroma. Association of cylindroma with desmoplastic trichoepithelioma demonstrate concurrent mutations within the CYLD gene. Nevertheless, absence of CYLD genomic mutation indicates mutant functioning of alternative genes in the emergence of desmoplastic trichoepithelioma. Desmoplastic trichoepithelioma predominantly arises within zones of sun exposure and can simulate lesions of basal cell carcinoma 1, 2.
Clinical Elucidation
As desmoplastic trichoepithelioma occurs within areas of sun exposure, preponderantly right sided facial zones such as the cheek, nose, chin, lips, mandible, periorbital region, eyebrow and forehead are implicated although the tumour can infrequently be situated upon upper trunk, neck and scalp 2.
Desmoplastic trichoepithelioma is an asymptomatic, solitary, well circumscribed, gradually evolving, flesh coloured or yellowish, firm to hard, indurated, plaque, papule or a nodule confined principally to the dermis. The lesion delineates an annular margin and a depressed, crater-like, non ulcerated centric zone, a diffuse pattern of tumour evolution, foci of peri-neural invasion (PNI) and basaloid cords and cellular nests embedded within a fibrous tissue stroma. An estimated 70% instances exhibiting peri-neural invasion are devoid of tumour reoccurrence. The lesion is devoid of pain, itching, ulceration, secondary lymph node enlargement or associated symptoms. Incriminated family members can demonstrate a nodular basal cell carcinoma in concurrence with desmoplastic trichoepithelioma. Combined lesions can arise upon the forehead and appear as a flesh coloured, poorly defined plaque 2, 3.
Histological Elucidation
Desmoplastic trichoepithelioma is challenging to discern on clinical and histological grounds, especially when evaluated with miniature, superficial, shave tissue samples. Thus, deep-seated tissue sampling is required. Brownstein and Shapiro in 1977 delineated the morphological features of desmoplastic trichoepithelioma as configuring narrow strands of basaloid tumour cells, keratinous cysts and an encompassing desmoplastic stroma. Aforesaid features exemplify a unique histological triad categorizing desmoplastic trichoepithelioma. Enunciation of a thin walled, attenuated epidermis and an absence of superficial telangiectasia assists the discernment of desmoplastic trichoepithelioma 3, 4.
On gross examination, frequently the tumours are gradually progressive, grey/white or flesh coloured, indurated, non ulcerated with a central depression and a magnitude varying within a few millimetres. The well circumscribed lesion is symmetrical, confined to papillary dermis and upper two thirds of reticular dermis. Emergence of narrow strands of basaloid epithelial cells, numerous horn cysts, a dense, encompassing fibrous tissue stroma, foreign body granulomatous reaction, several foci of calcification and articulation of osteoma within the lesion provide diagnostic characteristics 3, 4.
Nests, strands and miniature cords of basaloid epithelial cells of variable dimension, encompassed within a dense fibrotic tissue stroma are observed within the upper and mid-dermis. Cellular aggregates are rimmed with collagen bundles, multiple horn cysts appear within the stroma and a layering of stratified squamous epithelium is enunciated. Foci of calcification are apparent. Mitotic figures, peripheral palisading, apoptotic bodies aggregated within the epithelium or cellular and nuclear pleomorphism are absent 3, 4
Commonly, miniature strands of basaloid cells are encompassed within a desmoplastic stroma in association with keratinous cysts, usually abutting or attached to basaloid cell aggregates. Superimposed epidermis demonstrates a mild atrophy in accompaniment with enlarged cords of tumour cells aggregated within the mid - dermis. Connective tissue hyperplasia is observed within the horn cysts 4, 5.
Lesions are generally superficial and infrequently invade lower dermis. Tendency for peri-neural or intra-neural infiltration, cogitated in adjunctive cutaneous carcinomas, is exceptional in desmoplastic trichoepithelioma. Nevertheless, desmoplastic trichoepithelioma can be exemplified as a component of particularly desmoplastic, cutaneous carcinomas demonstrating foci of peri-neural involvement 4, 5. Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Figure 6, Figure 7, Figure 8.
Figure 1. Desmoplastic trichoepithelioma demonstrating aggregates of basaloid cells with numerous keratinous horn cysts interspersed in an intensely fibrotic stroma 9.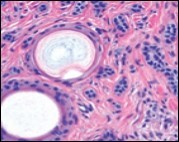
Download figure
Figure 2. Desmoplastic trichoepithelioma delineating cords and nests of basaloid cells, few horn cysts and a circumscribing fibrotic stroma 9.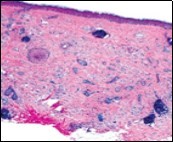
Download figure
Figure 3. Desmoplastic trichoepithelioma exhibiting accumulated basaloid epithelial cells disseminated amongst a background of abundant fibrous tissue stroma and an attenuated superimposed epidermis 10.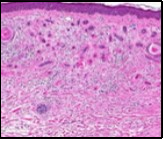
Download figure
Figure 4. Desmoplastic trichoepithelioma depicting cords and aggregates of basaloid epithelial cells with encompassing dense, compact fibrous tissue stroma 11.
Download figure
Figure 5. Desmoplastic trichoepithelioma enunciating several horn cysts, nests of basaloid cells, an enveloping desmoplastic stroma and thinned out superimposed epithelium 12.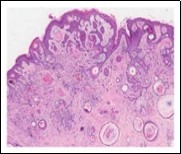
Download figure
Figure 6. Desmoplastic trichoepithelioma displaying few horn cysts, nests of basaloid cells and an abundance of desmoplastic, fibrotic stroma with an attenuated squamous epithelial lining 13.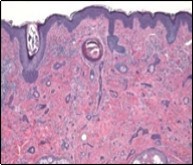
Download figure
Figure 7. Desmoplastic trichoepithelioma exemplifying several keratinous horn cysts, nests of basaloid cells, a desmoplastic fibrotic stroma along with a thinned out squamous epithelial lining 14.
Download figure
Figure 8. Desmoplastic fibrotic stroma demonstrating a thinned out, superimposed epithelium, fibrotic stroma and a dispersal of basaloid cell cords and aggregates 15.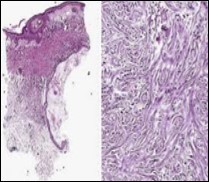
Download figure
Immune Histochemical Elucidation
A consistent immune reaction of cytokeratin 20 (CK20) is enunciated by Merkel cell, accompanied by a circumscription of stromal cells. Immune reactivity to cytokeratin 20(CK20) varies from intense to minimal and appears within few to multiple cells. Also, epithelial cells immune reactive to cytokeratin 20 (CK20) are diffusely dispersed within strands of tumour cells and horn cyst walls. Epithelial cells immune reactive to CD34+ are found to envelop the tumour cell mass. Epithelial membrane antigen (EMA) and androgen receptor (AR) are immune non reactive. Bcl-2 is weakly immune reactive within the basal layer 4, 5.
Immune reactions differentiating desmoplastic trichoepithelioma from morphea-like basal cell carcinoma (MBCC) are reactivity for cytokeratin 20 (CK20) highlighting Merkel cells, p53, p75, CD10, CD34, pleckstrin homology like - domain family A member 1 (PHLDA1), androgen receptors (AR), proliferative index with Ki-67 and Bcl2. Assessment of reactive CD20 and androgen receptors are superior in segregating desmoplastic trichoepithelioma from morphea-like basal cell carcinoma whereas evaluation of Ki-67 and Bcl2 may not be advantageous or confirmatory 4, 5.
Differential Diagnosis
Desmoplastic trichoepithelioma can clinically and histologically recapitulate several benign and malignant conditions such as syringoma, morphea-like basal cell carcinoma (MBCC), microcystic adnexal carcinoma (MAC), conventional trichoepithelioma and adjunctive tumours. Additionally, sebaceous hyperplasia, granuloma annulare, scar tissue, hamartoma, melanocystic nevi, keratosis and cutaneous squamous cell carcinoma require a demarcation. Histological differentiation is mandated from morphea-like basal cell carcinoma (MBCC), microcystic adnexal carcinoma (MAC) and eccrine syringo-carcinoma 5, 6.
Morphea-like basal cell carcinoma (MBCC) or sclerosing basal cell carcinoma is an aggressive, exceptional variant with an atypical clinical representation. It emerges as a solitary, yellowish, pale or flesh coloured, firm, poorly-defined, waxy or scar like, flat or mildly depressed lesion predominantly appearing on the head and neck, face, trunk, limbs and aforesaid lesions clinically and histologically recapitulate benign desmoplastic trichoepithelioma. Basal cell carcinoma preponderantly appears as nodular or superficial. As an aggressive subtype, morphea-like basal cell carcinoma therapeutically necessitates complete surgical excision, in contrast to benign desmoplastic trichoepithelioma. As aforesaid tumours are predominantly composed of follicular germinative cells, several common morphological characteristics can concur 6, 7.
Akin to desmoplastic trichoepithelioma, morphea-like basal cell comprises of infiltrating strands and islands of basaloid and monomorphic epithelial cells embedded within a dense fibrous and sclerotic stroma. Five distinct histological features aid the differentiation of desmoplastic trichoepithelioma from morphea-like basal cell carcinoma such as the occurrence of annular lesions, horn cysts, epidermal hyperplasia, keratin granules and calcification. Enlarged aggregates of tumour cells are frequent in morphea-like basal cell carcinoma and exceptional in desmoplastic trichoepithelioma. Syringoma is a benign, predominantly pubertal, cutaneous adnexal tumour demonstrating ductal differentiation and manifests miniature, asymptomatic, multiple, flesh coloured papules preponderantly situated upon cheeks, lower eyelids or periorbital region 6, 7. On histology, synrigoma delineates multiple eccrine ducts, doubly layered with cuboidal epithelium, scattered within dermal fibrous tissue stroma. Several, engendered tubular articulations are generally confined to the superficial dermis. Features such as narrow cords and strands of basaloid cells, foreign body granulomas and calcification are exceptional in syringomas although frequent in desmoplastic trichoepithelioma 6, 7.
In contrast, predominantly solitary with a lack of ductal differentiation, desmoplastic trichoepithelioma commonly displays horn cysts, calcification, follicular differentiation and elongated epithelial strands. Immune reactivity for cytokeratin 20 (CK20) for Merkel cells and non reactivity for carcinoembryonic antigen (CEA) is nearly comprehensive in desmoplastic trichoepithelioma, a pattern which is reversed in luminal cells of syringoma. Microcystic adnexal carcinoma is an exceptional adnexal neoplasm commonly arising upon centroidal face or head and neck region. A gradually evolving, enlarged, asymmetrical, firm, flesh coloured, indurated, diffuse plaque or nodule with poorly defined perimeter, demonstrating occasional, superimposed telangiectasia and extension into subcutaneous adipose tissue is exemplified 6, 7.
Microcystic adnexal carcinoma (MACs) as an exceptional, cutaneous carcinoma, invades locally and metastasizes infrequently. Indolent, flesh coloured or yellowish, facial lesions of MACs demonstrate basaloid cellular cords and nests embedded within a fibrous tissue stroma. MACs are diffuse lesions, infiltrate the subcutaneous tissue and depict perineural invasion (PNI) in around 80% instances. A singular immune stain segregating trichoepithelioma from a microcystic adnexal carcinoma is absent 6, 7.
Histologically, predominantly proliferating tubular articulations are denominated. In contrast to a benign, indolent desmoplastic trichoepithelioma, microcystic adnexal carcinoma is aggressive and displays significant localized tissue destruction and possible distant metastasis. Superficial extraction of tissue samples can result in misinterpretation of microcystic adnexal carcinoma as a squamous cell carcinoma, syringoma or desmoplastic trichoepithelioma in an estimated 30% instances 6, 7.
Immune reactivity to cytokeratin 20 (CK20), cytokeratin 15(CK15) and cytokeratin 7(CK7), CD10 and BerEp4 can be employed to segregate microcystic adnexal carcinoma from desmoplastic trichoepithelioma although none is confirmatory. Familial instances of MACs can concur with basal cell carcinoma or a papillary carcinoma thyroid.
Cutaneous metastatic breast carcinoma requires distinction from desmoplastic trichoepithelioma. Majority of cutaneous metastasis from carcinoma breast are enunciated following detection of the primary carcinoma. Infrequently, metastasis can be discovered prior to or concurrent with primary breast carcinoma. Breast carcinoma is a malignancy frequently delineating cutaneous metastasis. An estimated 30% of breast cancers exemplify a tendency to metastasize. Common sites of cutaneous metastasis of carcinoma breast are chest and abdomen. Infrequently, metastatic lesions can be cogitated upon scalp, face, neck, upper, extremities, ventral trunk. Rapidly enhancing, asymptomatic, firm, scar - like nodules or facial tumefaction can simulate desmoplastic trichoepithelioma. Nevertheless, cutaneous metastasis from a primary breast cancer requires diagnostic exclusion 5, 7.
Investigative Assay
Genetic assay delineates non reactive incriminated coding exons of CYLD gene extracted from deoxy ribo nucleic acid (DNA) of peripheral blood lymphocytes of blood relatives. Genetic concurrence betwixt desmoplastic trichoepithelioma, microcystic adnexal carcinoma and basal cell carcinoma requires further evaluation 1, 2.
Therapeutic Options
Desmoplastic trichoepithelioma enunciating foci of perineural invasion can be managed with conservative measures. Alternatively, a comprehensive surgical excision is beneficial and is accompanied by a lack of tumour reoccurrence 7, 8.
Moh’s micrographic surgery can be adopted. Regular follow up and antecedent tissue examination procures an early diagnosis with minimal cosmetic encumbrance. Enlarged lesions with peri-neural invasion mandate an appropriate monitoring to assess clinical behaviour. An aggressive therapeutic approach should be adopted with caution, similar to associated cutaneous carcinomas, especially for treating lesions situated upon cosmetically sensitive lesions 7, 8.
Moh’s micrographic surgery can be adopted for managing desmoplastic trichoepithelioma in order to circumvent tumour reoccurrence and localized tissue invasion as aggressive behaviour is extremely exceptional. Moh’s micrographic surgery is beneficial in treating lesions of atypical histology or appearing in sensitive zones, as the face or areas necessitating tissue sparing surgery. However, micrographic surgery remains an expensive therapeutic option, in contrast to alternative surgical procedures 7, 8.
Therapeutic modalities such as laser surgery, dermabrasion, administration of topical 5% imiquimod, curettage, electrodessication and radio-surgical abrasion can be employed to manage desmoplastic trichoepithelioma, although proportionate reoccurrence is enhanced with aforesaid techniques, as apposed to localized surgical extermination. Majority of superficial tissue samples are accompanied by inferior pathological evaluation. Thus, as aforesaid techniques may not be competent in procuring a histologically adequate tumour margin, evaluation of aggressive tumours simulating desmoplastic trichoepithelioma may not be satisfactory7, 8.
Localized surgical extermination of the lesion is a preferential treatment for a majority of benign tumours. Comprehensive remission with minimal reoccurrence of can be achieved with surgical methods although post- surgical complications such as scarring and hypopigmentation can occur in cosmetically sensitive zones as the face. Classic, definitively benign lesions of desmoplastic trichoepithelioma can be satisfactorily managed with close monitoring, regular follow up and localized surgical excision 7, 8. (Table 1)
Table 1. Differential Diagnosis of Desmoplastic Trichoepithelioma 1.| Features | Desmoplastic Trichoepithelioma | Syringoma | Cutaneous Metastasis Carcinoma Breast | Morphea -like basal cell carcinoma | Microcystic adnexal carcinoma |
| Narrow strands of basaloid tumour cells | Constant | Unusual | Rare | - | - |
| Hard, annular lesion | Typical | Rare | Negative | Rare | - |
| Horn Cysts | Constant | Rare | Rare | Rare | - |
| Solitary tumours | Common | Rare | - | - | - |
| Epidermal Hyperplasia | Common | Rare | Rare | - | - |
| Ductal Differentiation | Rare | Common | - | - | Frequent |
| Foreign body granuloma | Frequent | Rare | Rare | - | - |
| Calcification | Frequent | Rare | Rare | Infrequent | - |
| Periorbital involvement | Rare | Common | - | - | - |
| Symmetry | Often symmetrical | - | - | Often asymmetrical | Asymmetrical |
| Chest involvement | Negative | - | Common | - | |
| Large masses of tumour cells | Never | - | Common | Common | - |
| Cellular atypia | Never | - | Common | - | - |
| Ulceration | Rare | - | - | Common | - |
| Central depression | Common | - | - | Uncommon | - |
| Collagen rimming | Constant | - | - | Infrequent | - |
| Strands of epithelium | Frequent | - | - | Infrequent | - |
| Intramuscular, perichondrial and perineural involvement | Uncommon | - | - | - | Common |
| Circumscription | Well circumscribed | - | - | - | Poorly circumscribed |
| Infiltration | Confined to papillary dermis and upper two thirds of the reticular dermis | - | - | - | Extending beyond the reticular dermis |
References
- 1.Wang Q, Ghimire D. (2015) Desmoplastic Trichoepithelioma : a clinico-pathologic study of three cases and review of literature Onco. , Lett 10(4), 2468-2476.
- 2.Lovgren M L, Rajan N. (2019) Inherited desmoplastic trichoepitheliomas Clin Exp Dermatol. 44(7), 238-239.
- 3.Mamelak A J, Goldberg L H. (2010) A desmoplastic trichoepithelioma. , J Am Acad Dermatol 62, 102-106.
- 4.Moynihan G D, Skrokov R A. (2011) Desmoplastic trichoepithelioma. , J Am Acad Dermatol 64, 438-439.
- 6.Khelifa E, Masouye I. (2013) Dermoscopy of desmoplastic trichoepithelioma reveals other criterion to distinguish it from basal cell carcinoma. , Dermatology 226, 101-104.
- 7.Abbas O, Richards J E. (2010) Fibroblast-activation protein: a single marker that confidently differentiates morpheaform/ infiltrative basal cell carcinoma from desmoplastic trichoepithelioma. , Mod Pathol 23, 1535-1543.