
Melanoma of the Breast with Smoothened (SMO) Mutation: Case Report and review of the Literature
Abstract
We report the case of a 75 year-old female with past history of ampullary adenocarcinoma presenting with a rapidly enlarging breast mass, initially misclassified on fine needle aspiration as a probable sarcoma, which was ultimately diagnosed as melanoma on resection in the absence of a known cutaneous primary lesion. Next-generation sequencing (NGS) of the tumor revealed a mutation in the Smoothened oncogene (SMO) of unknown significance and wild-type BRAF. To our knowledge, SMO mutation in melanoma of any site has not been previously reported, though the effectiveness of SMO inhibitors has been studied in both in vivo and in vitro models of melanoma. Currently, these inhibitors have not been studied in SMO mutant melanoma. The patient declined further therapy after resection due to multiple comorbidities. She expired two years after presenting with the breast mass from complications of high grade urothelial carcinoma.
Article Information
- Received
- Accepted
- Published
Academic Editor: Xi Zhang, Research Assistant Professor, Feinberg School of Medicine, Northwestern University, United States.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Jennifer L. Clark, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Corresponding author: Ashraf Khan, Dept. of Pathology, UMass Memorial Medical Center, Three Biotech, One Innovation Drive, Worcester, MA 01605, USA —
Competing Interests
The authors have declared that no competing interests exist.
Funding
Data Availability
No data-availability statement was provided by the authors.
Acknowledgements
We would like to acknowledge Dr. Ediz Cosar for his guidance regarding the interpretation of molecular findings.
Citation:
Introduction
Melanoma is one of the most common non-hematologic metastatic tumors to the breast, second only to lung carcinoma1, 2, 3. However, the debate regarding the possibility of primary melanoma of the breast in the absence of a primary cutaneous lesion at another site is ongoing and remains controversial4,5. In general, particularly in the absence of continuous involvement with the skin or nipple, melanomas of the breast are thought to represent distant metastases in the majority of cases even when no primary lesion can be identified4. This debatable assumption has presented some difficulty in the surgical, chemotherapeutic, and radiotherapeutic management of these patients.
The diagnosis of melanoma in the breast is frequently difficult. Epithelioid melanomas may be mischaracterized as triple negative ductal carcinoma based on routine immunohistochemistry4. As in the present case, a melanoma with spindle cell features might be mistaken for a high grade sarcoma based on absent cytokeratin expression4. Several case studies have reinforced the importance of considering this diagnosis on biopsy and/or cytology specimens when there is absent expression of cytokeratin and hormone receptors4, 6, 7, 8. The role of molecular and genetic studies in the diagnosis and management of melanoma in the breast has not been well studied.
We report the case of a breast melanoma in a patient with no identifiable primary cutaneous lesion and unexpected molecular findings.
Case Report
We report the case of a breast melanoma in a 75-year-old woman with a cancer history significant for ampullary adenocarcinoma for which she underwent surgery and chemoradiation approximately 9 years earlier. She presented to her oncologist with a left breast lump which appeared suddenly. There was no axillary lymphadenopathy. Diagnostic ultrasound and mammography revealed a 3.3 cm solid mass at 12 o’clock deep to the areola which approached the skin (Figure 1). Fine needle aspiration was performed at that time which was positive for malignant cells, consistent with a high grade sarcoma or spindle cell type carcinoma (Figure 2A,B). The malignant cells were focally positive for GATA3 and negative for ER and PR, and this was thought to represent a primary breast cancer. A metastasis from her ampullary adenocarcinoma was ruled out immunophenotypically. The patient chose to undergo mastectomy for definitive diagnosis and treatment.
Figure 1. Radiological Findings. Radiographic imaging of the breast revealed a heterogeneous, hypoechoic solid mass with vascularity measuring 3.3 cm with associated thickening of the skin. A. Tomography, B. Ultrasound 
Download figure
Figure 2. Histopathological Findings. Fine needle aspiration revealed spindled, pleomorphic cells with numerous mitoses and apoptotic bodies. The cells were negative for cytokeratins and markers of breast, gastrointestinal, and hepatobiliary differentiation. Microscopic examination of the resected tumor revealed a poorly differentiated neoplasm with predominantly spindled morphology and diffuse expression of markers of melanocytic differentiation. A. Thinprep (40x), B. Cell block (H&E, 20x), C. H&E (10x), D. H&E (40x), E. Pan-cytokeratin (10x), F. GATA3 (10x), G. S100 (10x), H. SOX 10 (10x).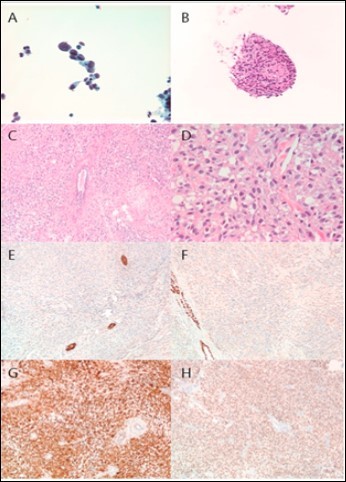
Download figure
A mastectomy was performed without lymphadenectomy. Pathological examination revealed an irregularly shaped, homogenous tan/white mass which closely approached but did not involve the overlying skin. Immunohistochemical analysis revealed negativity for cytokeratins, EMA, myoepithelial markers, GATA3, mammaglobin, ER, and PR. The tumor cells were diffusely positive for S100, SOX10, and MITF1 and focally positive for HMB45, Melan-A, and MART-1. A diagnosis of malignant melanoma involving the breast was rendered (Figure 2C-H). The skin was entirely submitted, and no evidence of melanoma in situ or dermal lymphatic involvement was identified. Molecular characterization by next generation sequencing (NGS) revealed wild-type B-RAF, c-KIT, and N-RAS. However, the tumor was found to harbor a Smoothened oncogene (SMO) I408M substitution (gene locus 7q32.1), a mutation of uncertain significance in melanoma. A TP53 inframe deletion, a previously confirmed somatic mutation, was also identified. Sequencing of benign tissue from the same patient revealed no evidence of the SMO mutant, consistent with somatic origin.
As the patient had no previous history of malignant melanoma, a search for a cutaneous primary was undertaken. She underwent a complete skin examination which revealed no suspicious lesions. Full body PET and MRI of the brain revealed no evidence of metastatic disease. Given the patient’s comorbid conditions, she opted for periodic surveillance and declined chemotherapy and radiation treatment. Unfortunately, the patient was subsequently diagnosed with a high grade papillary urothelial carcinoma involving the right ureter with associated obstruction. Subsequent imaging showed masses in the liver and T12 vertebral body suspicious for metastatic disease, but no biopsies were obtained. The patient expired secondary to progressive renal failure nearly two years after presenting with a breast mass. An autopsy was not performed.
Materials and Methods
Fine needle aspiration of the lesion was performed by the surgeon and the resulting aspirate entirely submitted in Cytorich Red. One ThinPrep slide was prepared and stained using the Papanicolaou technique on the automated Sakura Tissue-Tek Prism stainer (Sakura Finetek, Torrance, CA). A Cellient (Hologic, Marlborough, MA) cell block was also prepared.
Paraffin-embedded cell block and breast resection tissue sections were prepared on glass slides and stained with hematoxylin and eosin on an automated stainer. Immunohistochemical stains were performed using the following commercially available antibodies: cytokeratin-OSCAR (Covance, Dedham, MA); cytokeratin-AE1/AE3 (Ventana, Tucson, AZ); cytokeratin-CAM5.2 (BD, San Jose, CA); EMA (Ventana); p63 (Ventana); smooth muscle myosin (Ventana); calponin (Ventana); GATA3 (Cell Marque, Rocklin, CA); mammaglobin (Zeta, Sierra Madre, CA); estrogen receptor (Ventana); progesterone receptor (Ventana); S100 (Ventana); SOX10 (Cell Marque); MITF1 (Ventana); HMB45 (Ventana); Melan-A (Ventana); and MART1 (Covance).
Next generation sequencing was performed on DNA extracted from formalin-fixed paraffin-embedded tissue. Library preparation for each sample was performed using Ion AmpliSeq Library Kit 2.0 and AmpliSeq Cancer Hotspot Panel v2 (Life Technologies, Carlsbad, CA) according to the manufacturer’s instructions. Patient DNA was used as a template to generate the amplicon library for sequencing hotspot mutations in 50 designated genes. Details on the hotspot mutations included in this panel are available in supplemental form (Supplemental Table 1). The DNA library was clonally amplified onto IonSpheres (ISPs), diluted, and subjected to emulsion PCR on the OneTouch 2 System (Life Technologies). Following enrichment, the enriched ISPs were then subjected to sequencing on an Ion 318 Chip using Ion Sequencing Kit v2 (Life Technologies) according to the manufacturer’s instructions. The average coverage depth is 2000x to 3500x with the goal of detecting a heterozygous mutation in a specimen with 5% tumor content.
Discussion
We present a case of breast melanoma without known primary, initially characterized as a sarcomatous lesion. The most interesting aspect of this case is the unexpected finding on molecular analysis of an SMO mutation, a recently studied drug target in melanoma and other cutaneous malignancies. Mutation of the BRAF V600 codon is the most common genetic aberration in cutaneous melanomas, found in 40-60% of cases9,10. Though no organized study has investigated the incidence of BRAF mutation in primary noncuatneous breast melanoma, a single case reported by Rassouli and Voutsadakis11, demonstrated V600E mutated BRAF. Drueppel, et al.5 report a case with wild-type BRAF. At present, no studies have investigated the incidence of SMO mutation in melanoma of any site.
Several recent studies have shown success in inhibiting growth of melanoma cells in both in vitro and in vivo experimental models using the selective SMO antagonist NVP-LDE22512, 13. SMO is downstream of GLI1, a mediator of the sonic hedgehog pathway which has been shown to be overexpressed in melanomas with BRAFV600E mutations12. Interestingly, the drug also inhibits melanoma cells with wild-type BRAF, as in the current case12. This raises the question whether this patient could benefit from treatment with an SMO inhibitor in the presence of an SMO mutation. To our knowledge, the effectiveness of SMO inhibition with NVP-LDE225 in inhibiting melanoma cells has not been studied in the presence of an SMO mutant. Furthermore, though the SMO inhibitors sonidegib (NVP-LDE225) and vismodegib (GDC-0449) have been approved for treatment of basal cell carcinoma, these drugs are not currently approved for melanoma 14.
This case also reinforces the importance of including melanoma in the differential diagnosis of breast lesions with cytokeratin and hormone receptor negativity. If melanoma is not considered and appropriate immunohistochemistry performed, the lesion may be mischaracterized as a sarcoma. Treatment will differ significantly for each diagnosis. In a series of 16 cases of breast melanoma diagnosed on cytology, particular features were identified that should trigger consideration of this diagnosis, including plasmacytoid cellular morphology, pseudopapillary architecture, spindle cells, pigmented cells, and cellular pleomorphism8. Discohesion, binucleation, and granular cytoplasm were also prominent features in most cases8.
Conclusion
In summary, we present a case of malignant melanoma in the breast without cutaneous primary which was mischaracterized as a sarcoma on fine needle aspiration (FNA) cytology, reinforcing the importance of considering this diagnosis in breast core biopsies and FNAs. In addition, we report the unexpected finding on molecular analysis of a potentially targetable mutation in SMO, a gene uncommonly mutated in melanoma. Future studies are warranted to examine the incidence of SMO mutation and its biological significance in the pathogenesis and treatment of melanoma.
References
- 1.Georgiannos S N, Chin J, Goode A W. (2001) Secondary neoplasms of the breast: a survey of the 20th Century. , Cancer 92, 2259-66.
- 3.Rosen P P. (2010) Breast Pathology: Diagnosis by Needle Core Biopsy. 3ed. Philadelphia: Wolters Kluwer;.
- 4.Bacchi C E, Wludarski S C, Ambaye A B. (2013) Metastatic melanoma presenting as an isolated breast tumor: a study of 20 cases with emphasis on several primary mimickers. Arch Pathol Lab Med. 137, 41-9.
- 5.Drueppel D, Schultheis B, Solass W. (2015) Primary malignant melanoma of the breast: case report and review of the literature. Anticancer Res. 35, 1709-13.
- 6.He Y, Mou J, Luo D. (2014) Primary malignant melanoma of the breast: A case report and review of the literature. Oncol Lett. 8, 238-40.
- 7.Kharmoum S, Mohamed M, Benhammane H. (2014) Conjonctival melanoma metastatic to the breast: a case report. , BMC Res Notes 7, 621.
- 8.Ribu D L, Shield P W, Bligh J F. (2012) The varied presentation of metastatic melanoma in fine needle aspiration cytology of the breast. Cytopathology. 23, 256-62.
- 9.Bruno W, Martinuzzi C, Andreotti V. (2017) Heterogeneity and frequency of BRAF mutations in primary melanoma: Comparison between molecular methods and immunohistochemistry. , Oncotarget 8, 8069-8082.
- 10.Satzger I, Marks L, Kerick M. (2015) Allele frequencies of BRAFV600 mutations in primary melanomas and matched metastases and their relevance for BRAF inhibitor therapy in metastatic melanoma. , Oncotarget 6, 37895-905.
- 11.Rassouli M, Voutsadakis I A. (2016) Primary Noncutaneous Malignant Melanoma of the Breast. The breast journal. 22, 688-91.
- 12.Jalili A, Mertz K D, Romanov J. (2013) NVP-LDE225, a potent and selective SMOOTHENED antagonist reduces melanoma growth in vitro and in vivo. PLoS One. 8-69064.