
Abstract
Cellulitis is an acute, spreading pyogenic inflammation of the dermis and subcutaneous tissue, usually complicating a wound, ulcer, or dermatosis. Inappropriate diagnosis of cellulitis is a problem and would need prospective rather than retrospective studies to quantify the extent. There is one national guideline for the management of patients with cellulitis. The aim of this study is to determine the validity of Crest guideline in the patients with non-facial cellulitis. This prospective cohort study was conducted on all Adult patients with cellulites who were admitted at Resole-Akram and Sina emergency department between November 2013 and January 2014. Based on admission duration, the patients were randomly divided into two groups including primary and secondary outcome, <24-hours or >24-hours admission, respectively. Out of 89 admitted patients, 55% were hospitalized over 24 hours and 20% of them had significant systemic symptoms. The most patients (n= 42) had either systemically ill or systemically well or class II followed by classes I (n=28), III (n=18), and IV (n=1). There was significant relevancy between age, fever, PR, infected organ, leukocytosis, diabetes mellitus, IUDA, human bite, and primary outcome.
In conclusion, factors associated with admission were age, presence of multiple comorbid conditions, diabetes mellitus, human bite, IUDA, infected organ, leukocytosis and fever. These results showed that the decision in the emergency department was mostly the same as Crest guideline and the prospection of admission and discharge of these patients was almost according to the educations of Crest guideline.
Author Contributions
Academic Editor: Ahmed El-Sabbagh, Mansoura University Hospital
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Mohsen Abbasi, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Cellulitis is an acute, spreading pyogenic inflammation of the dermis and subcutaneous tissue, usually complicating a wound, ulcer, or dermatosis. It is a common medical condition taking up a large number of occupied bed days in acute hospitals 1.Streptococcus pneumonia is the most common germ of cellulites 2. Cellulitis must be differentiated from oedema with blisters, lower leg eczema, acute venous problems including thrombophlebitis, deep venous thrombosis, and liposclerosis, and vasculitis 3, 4. Inappropriate diagnosis of cellulitis is a problem and would need prospective rather than retrospective studies to quantify the extent. The distinctive features, including the anatomical location of cellulitis and the patient's medical and exposure history, should guide appropriate treatment 1. There is one national guideline for the management of patients with cellulitis. The Clinical Resource Efficiency Support Team (CREST) guideline present to evaluate patient with cellulites, the guideline indicators have been changed over the times 5. These guidelines have been published by the CREST, which is a small team of health care professionals established under the auspices of the Central Medical Advisory Committee in 1988. The aims of CREST are to promote clinical efficiency in the Health Service, while ensuring the highest possible standard of clinical practice is maintained 5.
There is a relative lack of observational studies look at the effects of treating predisposing factors on the recurrence of cellulitis. Even though the Crest guidelines are much easier to apply in clinical practice, their validity has never been proven by a clinical study. Revise this guideline seems valuable because of the most frequency of cellulites and the large amount of expenditure on this issue. Because of higher frequency of cellulites, higher Health system expenses, and the complications, the aim of this study is evaluation of Crest guideline in the patients with cellulitis and provide a valid criteria to admit or discharge of patients with cellulites in emergency department and improve the disease outcome using them, and decreasing the complications and patient expenses and finally the Health system expenses.
Material and Methods
The Ethics Committee of Iran University of Medical Sciences approved the study and author group collected written informed consent from all patients. This prospective cohort study was conducted on all Adult patients with cellulites who were admitted at Resole-Akram and Sina emergency department (ED) between November 2013 and January 2014. All patients with a single painful and restorable molar indicating symptomatic irreversible pulpitis (i.e., a history of spontaneous pain for a few seconds to several hours, pain exacerbating with hot and cold fluids, radiating pain, or reproducible pain with cold testing) were included in the study. Inclusion criteria were patients aged between 18 to 100 who had ED diagnosis of non-facial cellulites. Patient data inducing age, sex, presence of disease including diabetes, sepsis history or insect bite, Co-morbidity conditions such as trauma were collected. All clinical variables were independently recorded by two data abstractors. Based on admission duration, the patients were randomly divided into two groups including primary and secondary outcome, <24-hours or >24-hours admission, respectively. All patients initially discharged home were tracked for 7 days within our hospital and clinic health system to assess for repeat ED visits related to the initial presentation. Patient data were analyzed using STAT13 analyzer and analyzer was blind to patient outcome. Severity was assessed and compared with a CREST guideline for the management of cellulitis in adults 5. The significance of any differences in adverse outcome by demographic variable (age, gender, comorbidity), management (appropriate antibiotics) or severity classification (CREST) was tested using Fisher’s exact test. Unvaried analysis using ki-square was done for univariate data and subsequent multivariate analysis by forward and backward multivariate regression model was performed. Finally the area under receiver operator characteristic curve was reported.
Results
Out of 89 admitted patients, 55% were hospitalized over 24 hours and 20% of them had significant systemic symptoms. The clinical variables included demographic information, medical history, physical examination findings, and laboratory results are presented in Table 1 and Table 2. The most patients (n= 42) had either systemically ill or systemically well or class II followed by classes I (n=28), III (n=18), and IV (n=1) (Table 3). Forty patients were discharged within 24 hours and other 59 patients admitted in ward. Ninety percent of the patients who were classed in mild class of Crest guideline underwent outpatient treatment. Seventy percent of the CREST class II and all Crest class III or IV patients were treated in a Critical Care Unit. No significant relationship between primary outcome were seen among the patients with respect to gender, abscess formation, blood culture, treatment, hypertension, cigarette smoking, trauma and foreign body (P>0.05) (Table 4). There was significant relevancy between age, fever, pulse rate (PR), infected organ, leukocytosis, diabetes mellitus, intravenous drug abuse (IUDA), human bite, and primary outcome (P<0.05) (Table 4). The area under the receiver operating characteristic curve was 89%. Ki- square and logistic regression were done and significantly relevance between primary outcome and Crest guideline criteria was confirmed (Figure 1).
Table 1. Characteristics of patients presented to the emergency department with cellulites| Sex | Age | Farer | Location | Abscess | Leukocytosis | History of cellulites | Artificial joints |
|---|---|---|---|---|---|---|---|
| M (59) 66.30% | 20-100 | Yes (32) 36% | UE (9) 10.10% | Yes (8) 9% | Yes (31) 34.80% | Yes (1) 1.10% | (1) 1.1% |
| F 30 33.70% | 18-90 | No (57) 64% | LE (80) 89.90% | No (81) 91% | No (58) 65.20% | No (88) 98.90% | (88) 98.9% |
| Medical history | Frequency | Percentage |
|---|---|---|
| Diabetes Mellitus | + (35), - (54) | + (39.9%), - (60.7%) |
| Hypertension | + (13), - (76) | + (14.6%), - (85.4%) |
| Smoking | + (27), - (62) | + (30.3%), - (69.7%) |
| IUDA | + (9), - (80) | + (10.1%), - (89.9%) |
| Surgery history of infected extremity | + (1), - (88) | + (1.1%), - (98.9%) |
| Trauma | + (20), - (69) | + (22.5%), - (77.5%) |
| Human bite | + (1), - (88) | + (1.1%), - (98.9%) |
| Insect or animal bite | + (2), - (87) | + (2.2%), - (97.8%) |
| Deep vein thrombosis | + (1), - (88) | + (1.1%), - (98.9%) |
| Foreign body | + (4), - (85) | + (4.5%), - (95.5%) |
| History of cellulitis | + (1), - (88) | + (1.1%), - (98.9%) |
| Artificial joint | + (1), - (88) | + (1.1%), - (98.9%) |
| Percent | Number | Classification of all patients |
| 31.46 | 28 casesDischarge(27)/admission(1) | Patients who had no signs of systemic toxicity or class I |
| 47.19 | 42 casesDischarge(13)/admission(29) | Patients who had either systemically ill or systemically well or class II |
| 20.22 | 18 casesAdmission (18) | Patients who had a significant systemic upset or class III |
| 1.13 | 1 caseAdmission (1) | Patients who had sepsis syndrome |
| Variables | P value | OR (CI 95%) |
|---|---|---|
| Age | 0.007 | 1.04 |
| Sex | 0.829 | 1.1 |
| Fever | 0 | 0.033 |
| PR | 0 | 1.08 |
| Infected organ | 0.02 | 3.46 |
| Blood culture | 0.34 | 1.22 |
| Abscess formation | 0.25 | 0.377 |
| Leukocytosis | 0 | 0.0608 |
| Treatment | 0.423 | 2.075 |
| Diabetes mellitus | 0 | 0.159 |
| Hypertension | 0.101 | 0.316 |
| IUDA | 0. 017 | 0.782 |
| Trauma | 0 | 3.12 |
| Human bite | 0.131 | 0.219 |
| Animal or insect bite | 0 | 2.206 |
| Foreign body | 0.43 | 0.793 |
Figure 1.Ki- square and logistic regression showed significantly relevance between primary out come and Crest guideline criteria.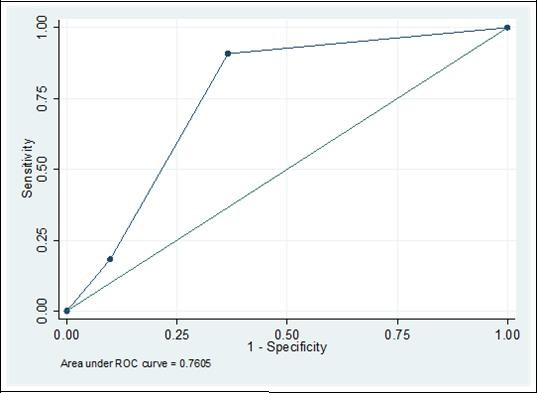
Discussion
The primarily aim of this study was to determine the validity of Crest guideline in the patients with non-facial cellulitis. Patients with facial cellulitis were excluded due to the potential complexity of these infections, proximity to the brain and vital structures, and difference in clinical management relative to soft tissue infections in other body regions 6. To our knowledge, this is the first prospective study that evaluated validity of Crest guideline in clinical observations. Our results show that all patients (100%) who had Crest guideline symptoms were hospitalized and most of the patients without these symptoms were discharged. Of the 89 patients initially admitted to the hospital, 40 were discharged under 24 hours. There were significant agreements between the primary outcome and Crest classifications for 96% of patients with mild disease or Crest class I. Seventy percent of the CREST class II patients and all Crest class III or IV patients were hospitalized. In this study, we have defined two different patient groups. The first group consists of patients who were discharged early (under 24 hour) without complications (low risk) and who accounted for 44.9% of the total. Another group of patients with cellulitis were delineated. The largest group (55.1% of patients) included those patients hospitalized for more than 24 hour. There has recently been a trend toward increasing the number of patients treated in the outpatient setting 7. However, the decision of whether to discharge or hospitalize a patient is difficult and is dependent on multiple factors 8, 9.
Of all the variables assessed in this study, fever and leukocytosis were the strongest predictors of prolonged admission. It has been demonstrated that fever is one potentially important factor (using either initial ED vital signs or patient history) in predicting the need for inpatient admission for patients presenting with nonfacial soft tissue infection 6, 10, 11.In this study patients with leukocytosis was also associated with a greater rate of hospital admission than those of had normal white blood cell count. This leukocytosis is likely reflective of more severe illness 11. It remains uncertain how emergency physicians would use this knowledge in the management of patients with skin infections or celliltis. However, Volz et al. (2013) suggested that leukocytosis is an important factor effective on primary outcome of patients with cellulitis 12.
Other variables which might intuitively be associated with a higher likelihood of admission such as diabetes (DB), age, PR, infected organ, IUDA, human bite, advanced age were significantly associated with admission. These findings are in similar to previous studies 10, 13. It has been demonstrated that patients with diabetes, the elderly and patients with peripheral vascular disease are at high risk of morbidity and mortality 14. Most of the patients (70%) who had co-morbidity or other conditions were admitted. These results are supported to previous study reported by Marwick et al 15. Carratala et al (2003) also suggested that co-morbid conditions increase the risk of complications in adults patients hospitalized for infectious cellulitis. Unlike prior study evaluating hospitalized patients with cellulitis found females to be associated with earlier discharge and a lower risk of death 16, there was no significant relationship between primary outcomes among the patients with respect to gender.
In conclusion, age, presence of multiple comorbid conditions, DB, human bite, IUDA, infected organ, leukocytosis and fever were factors associated with admission of patients with non-facial cellulitis. These findings can be used to stratify patients with acute cellulitis according to risks for complications and mortality and may be helpful when deciding the most appropriate means of care, i.e. outpatient treatment or hospitalization. These results showed that the decision in the emergency department was mostly the same as Crest guideline and the prospection of admission and discharge of these patients was almost according to the educations of Crest guideline.
References
- 2.Barzilai A, Choen H A. (1998) Isolation of group A streptococci from children with perianal cellulitis and from their siblings.Pediatr Infect Dis. , J 17, 358-60.
- 3.Tice A D. (1991) Once daily ceftriaxone outpatient therapy in adults with infections. Chemotherapy.37(Suppl3): 7-10.
- 4.Nathwani D. (2001) The management of skin and soft tissue infections: outpatient parenteral antibiotic therapy in the United Kingdom. , Chemotherapy 47, 17-23.
- 5. (2005) CREST(Clinical Resource Efficiency Support Team). CREST (Clinical Resource Efficiency Support Team) Guidelines on the Management of Cellulitis in Adults. DHSS Northern Ireland 1–31 .
- 6.Sabbaj A, Jensen B, Browning M A, John Ma O, Newgard C D. (2009) Soft tissue infections and emergency department disposition: predicting the need for inpatient admission. Acad Emerg Med. 16(12), 1290-1297.
- 7.Tice A D. (1995) Experience with a physician-directed, clinicbased program for outpatient parenteral antibiotic therapy in the USA. , Eur J Clin Microbiol Infect Dis 14, 655-661.
- 8.Fine M J, Auble T E, Yealy D M, Hanusa B H, Weissfeld L A et al. (1997) A prediction rule to identify low-risk patients with community acquired pneumonia. , N Engl J Med336: 243-250.
- 9.Rosón B, Carratalà J, Dorca J, Casanova A, Manresa F et al. (2001) Etiology, reasons for hospitalization, risk classes, and outcomes of community-acquired pneumonia in patients hospitalized on the basis of conventional admission criteria. , Clin Infect Dis 33, 158-165.
- 10.Moran G J, Krishnadasan A, Gorwitz R J, Fosheim G E, McDougal L K et al. (2006) Methicillin- resistant S. aureus infections among patients in the emergency department. , N Engl J Med 355(7), 666-674.
- 11.Shrock K J, Laskey S, Cydoka K R. (2008) Predicting observation unit treatment failure in patients with skin and soft tissue infection. , Int J Emerg Med 1, 85-90.
- 12.Volz K A, Canham L, Kaplan E, Sanchez L D, Shapiro N I et al. (2013) Identifying patients with cellultis who are likely to require inpatient admission after a stay in an ED observation unit. , Am J Emerg Med 31(2), 360-364.
- 13.Koerner R, Johnson A P. (2011) Changes in the classification and management of skin and soft tissue infections. , J Antimicrob Chemother 66(2), 232-234.
- 14.Montalto M, Davies F, Marijanovic N, Meads A. (2013) Skin surface temperature: a possible new outcome measure for skin and soft tissue infection. Aust Fam Physician. 42(9), 653-657.