
Abstract
Enteroatmospheric fistula is a challenging and emerging clinical situation, mainly related to “open abdomen” technique in damage control surgery for trauma and in case of multiple laparotomies.
We report the case of a 61-year-old male patient, affected by rectal carcinoma, submitted to standard surgical treatment and gradually evolving in persistent proximal jejunal fistula.
The positioning of a cardiac septal occluder (Amplatzer®) was associated with immediate and late favourable effects.
The procedure was conducted “bed-side” and turned out to be easy and safe.
Author Contributions
Academic Editor: Basem Azab, Staten Island university hospital
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Floriana Basiricò, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Enteroatmospheric fistula (EAF) is a challenging clinical situation: the increasing frequency that is observed and reported worldwide is mainly correlated to the “open abdomen” technique1, 2: this technique is used in damage control surgery for trauma and in patients submitted to multiple laparotomies3, 4 .
EAF is defined as a single or multiple communications between the visceral lumen and the atmosphere: EAFs (enteroatmospheric fistulas) are superficial or deep depending on the origin of the fistulas.
Standard treatment of EAFs includes:
·Drainage of the output
·Total parenteral (TPN) and/or enteral (TEN) nutrition
·Prevention and control of infection and sepsis
The management of such patients is typically made in Intensive Care Units (ICU) but, in spite of all the above therapies spontaneous closure is extremely unlikely; consequently the morbidity and the mortality are very high, often in association with a long hospitalization.
Furthermore, a “road map” is needed for an accurate definition of the number and site of EAFs5, using radiologic techniques, computed tomography (CT), fistulography and oral or nasogastric ingestion of charcoal or dye.
Figure 1.Nitinol occluder system (Amplatzer®)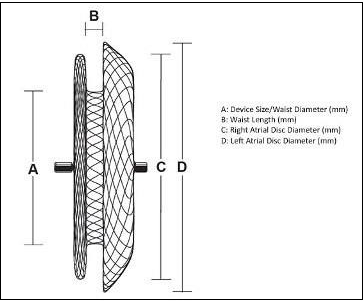
Figure 2.Nitinol occluder system (Amplatzer®)
Despite many adopted surgical and non-surgical techniques, a fully satisfactory method to treat this type of fistulas has not yet been described.
The aim of this study is to present a new technique to attempt the closure of an EAF by the positioning of a nitinol occluder system, a self-expandable double-umbrella-shaped device made of a nickel-titanium alloy (Figure 1, Figure 2).
Materials and Methods
A 61-year-old male patient, affected by rectal carcinoma, underwent a open standard anterior rectal resection. The postoperative course was particularly complex including postoperative haemorrhage, intestinal obstruction and perforation with the final arising of a jejunal multirecurrent EAF. The multistep treatment included many laparotomies with drainage, jejunal resections, direct closure of the EAF and “fistula- VAC” treatment; during a prolonged hospitalization in ICU, TPN and antibiotic therapy were associated. Despite of the several adopted treatments, the final result was a persistent proximal jejunal EAF surrounded by granulation tissue in the site of multiple laparotomies (Figure 3). The fistula output was 500 ml/day.
Figure 3.Enteroatmospheric fistula
So we positioned a Nitinol device (Amplatzer® Septal Occluder 18 mm)6 inside the EAF; such positioning was conducted “bed-side” without anaesthesia and proved to be easy and safe. The distal disk was introduced inside the jejunal lumen and the proximal disk was secured to the surrounding granulation tissue, utilizing the Nitinol’s super-elastic properties for the initial and progressive adaptation to the defect and the subsequent release (Figure 4).
Figure 4.Enteroatmospheric fistula with cardiac septal occlude
Immediately after the positioning of the device, a standard low-pression VAC therapy was started.
At time of positioning of Nitinol device, the patient was recovered in ordinary unit, not in ICU.
Results
We observed immediate rehabilitation, a better control of fecal output, so a standard oral nutrition was started in 7 days and TPN was discontinued in 15 days.
The patient demonstrated impressive early improvement in general condition and quality of life, particularly from the nutritional and psychological point of view.
VAC was effective with drainage of enteric fluide (50-100 cc/day) and progressive healing of the surrounding tissues; about ¾ of the device was inglobed in these tissues, with the remaining ¼ responsible for the intestinal leakage drained into the reservoir.
Finally the patient was discharged with a standard VAC therapy.
The device is still in place a 3 months, with gradually reduced output from the fistula and initial healing of the surrounding tissues.
Discussion and Conclusion
Various technique aimed at controlling effluent and allowing healing in patients with EAF have been reported within the last years7, 8.
On rare case it is possible to close very small holes with a cellular human dermal matrix or autogenous split-tickness skin graft9, 10, but the probability of success is very low.
Some Authors described an alternative technique of management of EAF consisting in a collapsible fistula isolation device11 with a separation technique using negative pressure wound therapy /reticulated open cell foam on fistula with moderate to high output levels. This technique provides control of effluent reducing complications of sepsi and accelerate wound healing.
Subramaniam et al.12 reported a “floating stoma” method, according to plastic bags are sutured between the edges of fistulated bowel and skin; a controlled fistula resembling a stoma is formed, source management can be provided by a stoma bag and the peritoneal cavity is protected until the granulation of the viscera allows skin grafting.
An other technique is described by Verhaalen et al.13, consisting in isolation of enteric contents from the wound bed by utilising an air and fluid impermeable “ring/silo” within an NPWT (negative pressure wound therapy) system.
The other source of control technique in EAF is the “baby bottle nipple method” defined by Layton et al14.
The Amplatzer Nitinol device is routinely adopted in the percutaneous closure of congenital heart defects; many Authors described the adoption of this device or of similar ones in several clinical and experimental situations. The use of this device in esophagorespiratory fistulas is described by Rabenstein et al.15 and Green et al.16; Kouklakis et al.17 used the device for the closure of a gastro-jejuno-colonic fistula; Perretta et al.18 and Asakuma et al.19 used a similar device for the endoscopic closure of a gastrotomy in an animal model; Malespin et al.20 positioned the device for palliationof a malignant gastrocolic fistula.
In the near future, with advancement of the healing of surrounding tissue, we will evaluate the possibility of removing the device for spontaneous healing or surgical closure of the residual fistula.
In general definitive surgery is delayed from 6 to 12 months to have a soft abdomen and to decrease the risk of bowel injury. In this procedure, it is essential to resect the bowel segment communicating with the fistula, restore intestinal continuity and cover the bowel with well-perfused soft tissue21.
Usually, more than 3 months (and sometimes up to a year) are needed before conditions are ideal for proceeding with surgery.
However the application of such device in an EAF has not yet described and are necessary more applications and outcomes data to fully understand the potential indications and long-term outcome associated with this technique. In our patient was easy, safe and effective; the outstanding advantages were the immediate improvement the quality of life, the early realimentation and the possibility of hospital discharge.
References
- 1.S Di, Tarasconi A, Inaba K, Navsaria P, Coccolini F et al. (2015) Open abdomen with concomitant enteroatmospheric fistula: attempt to rationalize the approach to a surgical night mare and proposal of a clinical algorithm. , J Am Coll Surg 220(3), 23-33.
- 2.S Di, Villani S, Biscardi A, Giorgini E, Tugnoli G. (2011) Open abdomen with concomitant enteroatmospheric fistula: validation, refinements, and adjuncts to a novel approach. , J Trauma 71(3), 760-2.
- 3.Latifi R, Leppaniemi A. (2012) Complex abdominal wall defects and enterocutaneousfistulae in the era of biological mesh: did we make any real progress?. , World J Surg 36, 495-496.
- 4.Bjorck M, Bruhin A, Cheatman M, Hinck D, Kaplan M et al. (2009) Classification-important step to improve management of patients with an open abdomen. , World J Surg 33, 1154-7.
- 5.Polk T M, Schwab C W. (2012) Metabolic and nutritional support of the enterocutaneous fistula patient: a three-phase approach. , World J Surg 36, 524-33.
- 6.Crawford G B, Brindis R G, Krucoff M W, Mansalis B P, Carroll J D. (2012) Percutaneous atrial septal occluder devices and cardiac erosion: a review of the literature. Catheter Cardiovasc Interv.1;80(2):. 157-67.
- 8.Verhaalen A, Watkins B, Brasel K. (2010) Technique and cost effectiveness of enteroatmospheric fistula isolation. , Wounds 22(8), 212-7.
- 9.Sarfeh I J, Jakowatz J G. (1992) Surgical treatment of enteric ‘bud’ fistulas in contaminated wounds. A riskless extraperitoneal method using split-thickness skin grafts. , Arch Surg 127(9), 1027-30.
- 10.Girard S, Sideman M, Spain D A. (2002) A novel approach to the problem of intestinal fistulisation arising in patients managed with open peritoneal cavities. , Am J Surg 184(2), 166-7.
- 11.Heineman J T, Garcia L J, Obst M A, Chong H S, Langin J G et al. (2015) Collapsible enteroatmospheric fistula isolation device: a novel, simple solution to a complex problem. , J Am Coll Surg 221(2), 7-14.
- 12.Subramaniam M H, Liscum K R, Hirshberg A. (2002) The floating stoma: a new technique for controlling exsposed fistulae in abdominal trauma. , J Trauma 53(2), 386-8.
- 13.Verhaalen A, Watkins B, Brasel K. (2010) Techniques and cost effectiveness of enteroatmosfheric fistula isolation. , Wounds 22(8), 212-7.
- 14.Layton B, Dubose J, Nichols S, Connaughton J, Jones T et al. (2010) Pacifyng the open abdomen with concomitant intestinal fistula: a novel approach. , Am J Surg 199(4), 48-50.
- 15.Rabenstein T, Boosfeld C, Henrich R, Ell C. (2006) First use of ventricular septal defect occlusion device for endoscopic closure of an esophagorespiratory fistula using bronchoscopy and esophagoscopy. , Chest 130(3), 906-9.
- 16.Green D A, Moskowitz W B, Shepherd R W. (2010) Closure of a broncho-to-neoesophageal fistula using an Amplatzer Septal Occluder device. Ann Thorac Surg. 89(6), 2010-2.
- 17.Kouklakis G, Zezos P, Liratzopoulos N, Pitiakoudis M, Efremidou E et al. (2010) Billroth II gastrectomy complicated by gastrojejunocolonic fistulas, treated andoscopically with a cardiac septal defect closure device. , Endoscopy. 42 Suppl 2, 134-5.
- 18.Perretta S, Sereno S, Forgione A, Dallemagne B, Coumaros D et al. (2007) A new method to close the gastrotomy by using a cardiac septal occluder: a long-term survival study in a procine model. , Gastrointestinal Endoscop 66(4), 809-13.
- 19.Asakuma M, Perretta S, Allemann P, Cahill R, Dallemagne B et al. (2010) Multimedia article. Per-oral dual scope NOTES cholecystectomy in porcine model (with video). Surg Endoscop. 24(10), 264-5.
Cited by (6)
- 1.Maurya Neha Shree, Mani Ashutosh, 2023, Navigating Molecular Pathways: An Update on Drugs in Colorectal Cancer Treatment, Current Topics in Medicinal Chemistry, 23(30), 2821, 10.2174/1568026623666230614165548
- 2.Pei Xiao Meng, Wong Heong Ting, Ng Simon Siu Man, Leung Wing Wa, Wong Yee Ni, et al, 2023, The diagnostic significance of CDH17-positive circulating tumor cells in patients with colorectal cancer, Expert Review of Molecular Diagnostics, 23(2), 171, 10.1080/14737159.2023.2176223
- 3.Merchant Neha, Nagaraju Ganji Purnachandra, 2020, , , (), 1, 10.1007/978-981-15-5471-1_1
- 4.Helmy Maged. W., Ghoneim Asser I., Katary Mohamed A., Elmahdy Rana K., 2020, The synergistic anti-proliferative effect of the combination of diosmin and BEZ-235 (dactolisib) on the HCT-116 colorectal cancer cell line occurs through inhibition of the PI3K/Akt/mTOR/NF-κB axis, Molecular Biology Reports, 47(3), 2217, 10.1007/s11033-020-05327-4
- 5.Koveitypour Zahra, Panahi Farnoush, Vakilian Mehrdad, Peymani Maryam, Seyed Forootan Farzad, et al, 2019, Signaling pathways involved in colorectal cancer progression, Cell & Bioscience, 9(1), 10.1186/s13578-019-0361-4
- 6.Del Zotto Giulio, Bellio Gabriele, Bernardi Laura, Biloslavo Alan, de Manzini Nicolò, 2021, Use of the Amplatzer cardiac septal occluder to heal a recurrent high‐output chronic enteroatmospheric fistula, ANZ Journal of Surgery, 91(3), 10.1111/ans.16191