
Abstract
The prevalence of type-2 diabetes (T2DM) among Mexican-American older adults along the U.S.-Mexico border region is at epidemic proportions. Healthcare reform is trending toward long-term home-based management of chronic conditions. Under the Mexican cultural norm of familism, daily care for elders is also often provided by family caregivers whose competence levels may vary. Adherence to the prescribed medication regimen is critical to attainment of optimal glucose control. However, there is a startling lack of literature that addresses the link between family medication administration and care recipients’ health outcome. This paper explores the role of culture in medication administration by family caregivers of elders with T2DM from the perspective of caregiver capabilities and caregiving demands. A critical review of the literature offers suggestions to guide future studies.
Author Contributions
Academic Editor: Roman Kireev, PhD, Senior Researcher
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Hsueh-Fen S. Kao, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Mexican Americans are twice as likely to develop type-2 Diabetes (T2DM) as non-Hispanic Whites.1 In Texas, 34.8% of Hispanics 65 or older suffer from T2DM versus 17.0% of their non-Hispanic White counterpart.2 T2DM is exceedingly prevalent along the U.S.-Mexico border, where 1.2 million people bear the burden of T2DM and its related co-morbidities,3 ranking it the fifth leading cause of death in El Paso County.4 Despite technologic and pharmacologic advances, individuals with T2DM at age 50 years still have a life expectancy 8.5 years shorter than their counterparts without diabetes.5 Diet, physical activity, and medication have long been recognized as the three major strategies for diabetes management.1 While there is a great deal of literature on diet and physical activity assisted by families, there is virtually no research linking family care of medication administration to effects on glucose control outcomes in individuals with T2DM. Thus, the purpose of this review is to propose key variables in family medication administration for Mexican American older adults with T2DM through the lens of the Family Adjustment and Adaptation Response Model (FAAR)6 and propose future studies taking cultural home-based chronic care into consideration.
Culture and Family Caregiving
Mexican Americans highly value the family care for older adults. Caregiving is likely to take place within the cultural context of familism, in which family members may be trusted as caretakers. Among Mexican Americans this translates into a likelihood of the caregiver being a younger female family member, usually a daughter or daughter-in-law. 7, 8 The older adult may relinquish care decisions, including medication regimen management to the caregiver, but still expect to remain in authority. The dyadic relationship can foster or hinder quality care, and depends on the range of caregiver capabilities and demands. In addition, older adults with T2DM may experience age-related impairments in cognitive and physical function, resulting in the need for caregivers to administer the medications. Failure to address the caregiver-older care receipt dyad and culture may partially explain outcome disparities among this target population. Furthermore, the target population is expected to become the largest minority age group by 2019.9 However, the evidence base needed to identify culturally appropriate interventions that optimize the quality of home-based caregiver-managed medication administration is insufficient.8
Prevalence, Morbidity and Cost
The prevalence of diabetes is rising globally. By 2025, about half of those age 65 or over will have T2DM and almost 60% will be diagnosed by 2050.4 The expected increase is closely associated with increasing age: 220% for those ages 65-74, and 449% for those 75 or older.10 In 2008, diabetes reportedly accounted for about $174 billion in medical expenses and reduced national productivity11 and diabetes-related spending is expected to reach $336 billion in 2034.5 In addition, Medicare spending is expected to rise from $45 billion in 2009 to $171 billion by 2034.1@
Family-based caregiving support for T2DM is especially important in the El Paso (TX) community because this group has up to four-times greater risk for diabetes.13 The statistics show significant disparities among Mexican Americans: 1, 14
1. In some Texas-Mexico border counties, T2DM affects up to 50% of the Mexican American population over 35 years.
2. Diabetes onset occurs earlier in Mexican Americans than non-Hispanic Whites, with 3.2% of Mexican Americans being diagnosed between 18-44 years old, compared to 1.3% of their non-Hispanic White counterparts.
3. Diabetes is highly related to body weight and obesity rates, which are 74.6% and 73% in Mexican American men and women, respectively, compared to 71% and 57.6% in the non-Hispanic White counterparts.
4. Mexican Americans with T2DM exhibit higher fasting glucose, decreased insulin sensitivity, increased insulin-resistance, and more severe complications than their non-Hispanic White counterparts.
Medication Adherence and Glucose Outco mes
Medication administration should be consistent with the prescribed regimen.15 Glycated hemoglobin (HBA1c), which identifies the 8-12 week average plasma glucose concentration, is the gold standard for measuring glucose control.10 The goal of home-based care is to maintain an HbA1c less than 6% to signal stable glucose metabolism and to reduce or delay diabetes complications.16 Normal HbA1c outcomes also enhance subjective wellbeing.17 Hypoglycemic agents can reduce HbA1c by 0.5%- 2.0%.18 Uncontrolled or progressive glucose instability, however, requires a more complex medication regimen. Although adding insulin to the medication regimen increases the complexity of the prescribed treatment, insulin is highly effective, but is more costly and uncomfortable for the older adult.19
Poor medication adherence is common problem among older adults with T2DM20 and the quality of home-based care can have a positive or a negative impact on diabetes control.21 Thus, health-related social and economic factors (e.g., education, income) are important in measuring quality and outcomes in this population.22
Family Caregiving and Care Recipients’ Health Outcomes
Current studies tended to focus on either clinical, behavioral, and knowledge outcomes of individuals with diabetes,23 or burden of caregivers11 and the impact of financial strain24 on families. We propose that Mexican cultural norms, which stress the importance of familism (familismo) and respect (respecto),25 are worthy of study because of the disparity in prevalence and morbidity, and a lack of literature examining the effect of family care on care recipients’ health outcomes. Evidence on which to base best practices (including modifying variables that strengthen the dyadic caregiver-elder relationship) is critical to achievement of glucose control in home-based family care.
Family Adjustment and Adaptation Response Model
The Family Adjustment and Adaptation Response Model6 stresses the role of family caregiving capabilities and the demands of medication administration, and resulting outcomes in glucose control in the elderly care recipient with T2DM (Figure 1). This model highlights family caregivers as central to the older adult’s glucose control so balance between caregiving capabilities and demands can have a significant impact on glucose control outcomes in the older adult. Family caregiving capabilities include health literacy, social support, household dependent ratio and perceived mutuality. Family demands include medication complexity, medication adherence, and affordability. This model can be used to understand the contribution of culture as important underlying context in the family dynamics process and, ultimately, glucose control.
Figure 1.Mexican-American Family Care of Medication Administration for Older Adults with Type-2 Diabetes Using Family Adjustment and Adaptation Response Model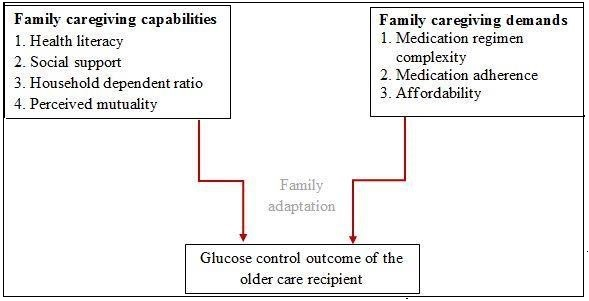
Methodology in Systematic Literature Review
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines in the development of this review. The aim of the PRISMA Statement is to improve reporting of systematic reviews and meta-analyses. Although PRISMA guidelines are primarily for systematic reviews of randomized clinical trials (RCTs), they can also be used for a systematic review of other types of research.26
PubMed and Cumulative Index to Nursing and Allied Health Literature (CINAHL) electronic databases were searched using five key words combined with the Boolean operator AND. Medical Subject Headings (MeSH) and keywords were used with searches in each database. The search strategy incorporated the following key terms: “Hispanic”, “family caregiving”, “medication”, “diabetes”, and “elders”. When the searches using these key words did not identify any articles, the key words were modified using “family caregiving”, “medication” and “elders”. When the search terms were expanded to include all chronic illness populations, the results yielded 14 and 3 articles from PubMed and CINAHL, respectively. One duplicate was eliminated; therefore, the total number of articles retrieved was 16. We reviewed published studies only, thus, no theses and dissertations were included. Two independent researchers reviewed the abstracts of the articles for relevance to the topic and eliminated 12; only four articles were retained and are included in this review.
The authors reached consensus on key variables that were most pertinent to Hispanic family caregivers and medication administration for older adults with T2DM--resulting in an alignment of the conceptualization of family caregiving with the FAAR model that stresses that the care recipient’s health outcomes are influenced by the balance between family caregiving capabilities and demands. Four key variables were selected to represent family caregiving capabilities (health literacy, social support, household dependent ratio, and perceived mutuality); three additional variables (medication regimen complexity, medication adherence, and affordability) were selected to signify family caregiving demands in Mexican American family medication administration for older adults with T2DM (see Table 1).
Table 1. Key Variables in Mexican-American Family Caregiving Capabilities and Demands related to Medication Administration for Older Adults| Family Caregiving related to Medication Administration | Key Variables | References |
| Caregiving Capacities | 1. Health Literacy | Bauer et al., 2013; Berkman et al., 2011; HealthyPeople.gov (2013); Hu et al. (2013); Pagan et al. (2012); Rothman et al. (2004); Wolf et al. (2014) |
| 2. Social Support | Gleeson-Kreig et a. (2002); Latham & Calvillo (2009); Trivedi et al. (2012) | |
| 3. Household Dependent Ratio | Kao et al. (2012); Rivera et al. (2009); Salas et al. (2009); U.S. Bureau of Census (2012 & 2013) | |
| 4. Perceived Mutuality | Kao & An (2012) | |
| Caregiving Demands | 1. Medication Complexity | Corsonello et al. (2009); McDonald et al. (2013); Thorpe et al. (2012); Tong et al. (2014) |
| 2. Medication Adherence | Ahmad at al. (2013); Farmer, Kinmonth, & Sutton (2006); Holland et al.(2010); Hong & Kang (2011); Odegard & Capoccia (2007); Odegard et al. (2013) | |
| 3. Affordability | Rivera et al. (2009); Centers for Medicare & Medicaid Services Chronic Condition Data Warehouse (2010); DHHS (2014); Office of Minority Health (2012); Rivera et al. (2009) |
Results
Family Caregiving Capabilities and Medication Administration
Mexican American family members are likely to assume the role of providing in-home diabetes care.27 Nonetheless, families vary in their ability to balance between capabilities and demands. Family capabilities to manage diabetes medication are a major determinant of whether the elderly care recipients suffer steady deterioration or remain in fairly stable health. Current literature focuses on these attributes among individuals with diabetes, and less on the attributes of their caregivers. While no family system measures were significant predictors of HbA1c in a small English speaking sample with T2DM,28 the results in Mexican American older adults with T2DM may be different due to various family cultural values and caregiving capabilities.
Health Literacy. The relationship between health literacy and health outcomes is well-documented29 and improving health literacy skills is an objective in Healthy People 2020.30 Special consideration is needed for Mexican American family caregivers along the U.S.-Mexico border,31 given the generally low educational attainment and low health literacy in this population. This suggests that Mexican American family caregivers’ health literacy is an important determinant of competence in medication administration. Caregiver competence in medication administration for older family members with T2DM is a priority in health care and education assessment. Needed skills include making judgments about dosage, as is required in a sliding scale insulin regimen.32 Additionally, the link between health literacy and HbA1c in individuals with diabetes has been established in the work of Wolf and colleagues16; other research, however, has failed to demonstrate this relationship.33 Few studies have explored the effects of the health literacy of family caregivers on the health outcomes of their elder recipients. This supports our proposition that family caregivers’ health literacy is an issue in home-based care of Mexican American elders with T2DM. Family caregivers with varying health literacy often play the role of mediator or translator for their aged family member during health care services so they may also need to be educated with related knowledge.
Social Support.
While having an important impact on the health outcomes of Mexican Americans, social support is a subjective concept that goes beyond merely counting the number of specific supports actually received.34 Among various conceptualizations, perceived social support is a good descriptor due to its significant associations with wellbeing, health outcomes, and family functioning.35 Although Gleeson-Kreig, Bernal, and Woolley36 stated that social support is not strongly related to T2DM self-care in Mexican American patients, the veracity of this argument is mitigated by the study’s small sample size and the fact that the authors affirmed the existence of a strong family support system in this culture. Social support embodies family caregiving capacities in medication administration within the cultural context of the Mexican American family.
Household Dependent Ratio.
Adult children who simultaneously support their younger children and older parents are colloquially known as the ‘sandwich generation’.37 This is especially true in the Mexican American family with strong cultural ties to Mexican culture, who also tend to have larger household sizes compared to Non-Hispanic white families.38 A higher household dependent ratio indicates that adult children are supporting dependents under 18 or over 65 years. The average household size in El Paso, TX, is 3.1 persons with 71% of households having one or more dependents,39 compared to an average household size of 2.6 persons in the general U.S. population, with 57.8% having one or more dependents—suggesting that Mexican American adult children are challenged to support a larger number of household dependents. Also, the cost of medication has been linked to lower medication adherence in patients with T2DM.20 Since T2DM is considered a long-term chronic condition, older adults may skip or decrease the dose of their medications. Also of note is the option of their family traveling to Juarez, Mexico (30 minutes away) to buy cheaper medications. Buying medications in Mexico may or may not be a good option since these prescription drugs are of undetermined quality and potency and may have a negative effect on the glucose control outcome.40
Perceived Mutuality.
Caregivers’ perceived mutuality from their older adult family member may affect the care provided. In a sample of Mexican American caregivers,41 cultural orientation was found to have minimal effect on filial attitudes and no significant effect on perceived mutuality, but perceived mutuality from and filial attitudes toward their older adult care recipients demonstrated a strong relationship. While caregivers with a strong Mexican cultural orientation tend to demonstrate a greater sense of filial obligation than do their Anglo-oriented counterparts, it is their perceived mutual equality with the older adult that demonstrates the most substantial effect on filial attitudes; thus ‘perceived mutuality’ may be a good predictor of quality of care and willingness to learn competency skills, translating to the care received by the elder with T2DM. In give-and-take family relationships, ‘you reap what you sow’ appears to be important to incorporate into studies of Mexican American family caregiving for older adults.41
Family Caregiving Demands and Medication Administration
Mexican American family caregivers are known to experience more barriers to administering medication than other ethnic groups.40, 42 Again, this is possibly due to the prevalence of lower educational levels and poorer understanding of English verbal and written instructions. Family demands may be risk factors interfering with medication administration for their older adults, especially when care recipients have a complex medication regimen, poor medication adherence, and inability to afford medications.
Medication Complexity.
A complex medication regimen affects the ability of both patients and their family to use medications correctly.43 The number of medications alone may not be the indicator of the complexity of a medication regimen. Adding to complexity, researchers have not yet reached a consensus on the most effective agent to treat T2DM.44 While many studies have provided information on efficacy of treatment, none have provided information on their impact on the clinical outcomes in older adults. Thus, it may be inappropriate to consider only the pharmacological effect of agents without considering family caregivers’ barriers in managing a complex medication regimen for their older adults.45
Medication Adherence.
In the past decade, the percentage of individuals over age 50 who used only insulin to treat diabetes declined significantly from 17 % in 1998 to 9% in 2008 but the use of oral agents, alone or combination with insulin, increased.46 This may be because an increased number of newly diagnosed older adults with diabetes are better controlled in the early stages with oral agents, diet, and exercise. Nevertheless, about 80% of older adults living with at least one chronic health condition require home-based medication administration,47 but inappropriate medication use is commonly reported in community-dwelling older adults. Studies of T2DM worldwide 48, 49 sowed a positive relationship between medication adherence and normal HbA1c levels. Also, 85% of patients using diabetes medications agreed that the medication was beneficial.50 Even adherence to diabetes medication was shown to be strongly related to HbA1c control.19 Diabetes medication adherence rates vary, however, from 31% to 98%.18 If older adults can adhere to their prescribed medication regimen, this can surely help family caregivers manage their medications.
Affordability.
Approximately 39.6% of Mexican Americans are uninsured,51 and the rate is even higher in El Paso— 40.4% (Rivera et al., 2009). Although the Affordable Care Act may positively impact these statistics, benefits may not reach a large portion of undocumented Mexican Americans and ironically, Medicare cuts have become a real possibility. Based on the Centers for Medicare and Medicaid Services Chronic Condition Data Warehouse,52 66.1% of older adults enrolled in Medicare Part D in 2007. Among them, only 9.6% were Mexican Americans despite poor older Mexican Americans’ eligibility for dual coverage with Texas Medicaid to bridge the drug accessibility gap. In fact, a lack of medication coverage drives one third of El Pasoans across the border to buy cheaper medications in Mexico.40 However, the crossing-boarder-purchase may be unsafe due to the possibility of less qualified health providers and counterfeit or sub-standard medications.
Conclusion
In this paper, the authors located several meaningful variables in Mexican American family caregiving capabilities and demands while providing care on medication administration for older adults through the lens of FAAR model. The variables related to family caregiving capabilities in medication administration include health literacy, social support, household dependent ratio, and perceived mutuality. The variables related to family caregiving demands include medication complexity, medication adherence, and affordability. Given the ever-increasing cost of care and longer life expectancy for older adults with diabetes, some researchers consider diabetes in the aged population to be the salient epidemic of the 21st century.12 Jacobson and Wood53 confirm that managing medications is one of the major caregiving tasks adult children perform for aged parents with diabetes. Due to various family dynamics, each caregiver-care recipient dyad should be individually assessed for the care. Administration of medications to older adults by family caregivers, may become more complex and could exert pressure on the family.54 In an era of health care reform and home-based care, the possibility of declining benefits for older adults translates into the imminent need to explore family caregiving competence in medication administration. It is expected that family caregiving for Mexican American elders with T2DM will continue to increase38 within the cultural mores of familismo and respecto. In conclusion, our critical review confirmed that Mexican American family caregiving competence in medication administration should be viewed using the lens of culture.
Limitations
The major limitation of this paper is, while common sense tells us that caregiving is for the greater good of care recipients, few literature links family care on medication administration to health outcomes of older care recipients. The authors recommend performing a systematic review in the relationship between family care on medication administration and health outcomes of care recipients on a regular base to include more updated studies in the review to conquer the lack of empirical evidence support.
Recommendations
In addition to aforementioned recommendation in performing a systematic review on the topic regularly, the authors also have the following suggestions: (1) older adults’ self-reported medication adherence should be compared with their primary caregivers’ report to avoid memory issues or socially desirable answers; (2) due to low literacy in this population, family caregivers should also be recipients of culturally appropriate information and education in medication administration to promote glucose control for older adults with T2DM; and (3) using the Medication Complexity Index, including the number, frequency, and special instructions for preparing medications, is suggested,55 to measure medication complexity. Even when the number of medications is low, the medication complexity may still be high with their associated frequency and instructions in taking medication.45
Summary
Although the population of aging Mexican Americans is expanding, few studies address caregiver competence in medication administration. A critical review of the literature on family care and medication administration for older adults noted several conceptual shifts in the past decade: (1) from common to diabetes-specific medication barriers: after a systematic review, Odegard and Capoccia18 concluded that factors affecting caregiving for individuals with diabetes include medication regimen complexity, dosing frequency greater than twice daily, cost, the need to remember doses and refills, and adverse effects; (2) from medication adherence to barriers: some researchers56 support the proposition that the most effective way to determine if Mexican Americans with T2DM are taking their medications as prescribed is to utilize negative proxy measurement to identify their non-adherence (i.e., measuring the barriers) in taking medication; and (3) from studying aged patients to studying their caregivers: it makes sense to shift study focus to family caregivers and the caregiver-care recipient dyad within cultural norms.57 The paper intends to draw healthcare researchers’ attention to this current but often neglected issue in family care of medication administration for older adults with diabetes.
References
- 1.American Diabetes Association. (2014) . Standards of medical care in diabetes-2014. Diabetes Care 37, 14-80.
- 2.Texas Diabetes Council (2012). Texas diabetes fact sheet. Retrieved from http://www.dshs.state.tx.us/diabetes/tdcdata.shtm
- 3.American Pan. (2007) Health Organization. Retrieved from http://www.diabeteshealth.com/read/2007/11/02/5549/diabetes-increasing-along-u-s---mexico-border/?isComment=1
- 4.Centers for Disease Control (2013) U.S.-Mexico border diabetes prevention and control project. Retrieved from http://www.cdc.gov/diabetes/programs/border.html
- 5.S M Lynch. (2010) Profiles of an aging society:. , Diabetes. Washington, DC:Gerontological Society of America
- 6.J M Patterson. (1988) Families experiencing stress: I. The Family Adjustment and Adaptation Response Model: II. Applying the FAAR Model to health-related issues for intervention and research. , Family Systems Medicine 6, 202-237.
- 7.Kao H F, McHugh M L, Travis S S. (2007) Psychometric tests of Expectations of Filial Piety Scale in a Mexican-American population. , Journal of Clinical Nursing 16, 1460-1467.
- 8.H F Kao. (2011) Medication administration hassles for Mexican American family caregivers of older adults. , Nuring and Health Sciences 13, 133-140.
- 9.DepartmentofHealthandHumanServices. (2010) A statistical profile of Hispanic older Americans aged 65+. Retrieved from http://www.aoa.gov/AoARoot/Aging_Statistics/minority_aging/Facts-on-Hispanic-Elderly.aspx
- 10.K M Narayan, Boyle J, Geiss L S, Saaddine J B, Thompson T J. (2006) Impact of recent increase in incidence on future diabetes burden: U.S.,2005-2050.Diabetes Care. 29, 2114-2116.
- 11.J H Lingler, Sherwood P, M H Crighton, M K Song, M B Happ. (2008) Conceptual challenges in the study of caregiver-care recipient relationships. , Nursing Research 57, 367-372.
- 12.E S Huang, Basu A, O’Grady M, J C Carpretta. (2009) Projecting the future diabetes population size and related costs for the U.S. Diabetes Care. 32, 2225-2229.
- 13.N C Martinez, Bader J. (2007) Analysis of behavioral risk factor surveillance system data to assess the health of Hispanic Americans with diabetes in El Paso County. , Texas, Diabetes Educator 33, 691-699.
- 14.NationalInstituteofDiabetes Digestive, KidneyDiseases. (2013) . Overweight and obesity statistics.Retrieved from http://win.niddk.gov/pub;ications/PDFs/stat904z.pdf
- 15.R W Grant, J A Schmittdiel. (2013) Adults with diabetes who perceive family members’ behaviour as unsupportive are less adherent to their medication regimen. , Evidence-Based Nursing 16, 15-16.
- 16.M S Wolf, Seligman H, T C Davis, D A Fleming, L M Curtis et al. (2014) Clinic-based versus outsourced implementation of a diabetes health literacy intervention. , Journal of General Internal Medicine 29, 59-67.
- 17.B A Levterova, Dimitrova D, G E Levterov, E A Dragova. (2013) Instruments for disease-specific quality-of-life measurement in patients with type 2 diabetes mellitus--a systematic review. , [Review]. Folia Medica 55, 83-92.
- 18.P S Odegard, Capoccia K. (2007) Medication taking and diabetes: a systematic review of the literature. , The Diabet Educatior 33, 1014-1029.
- 19.P S Odegard, Carpinito G, D B Christensen. (2013) Medication adherence program: adherence challenges and interventions in type 2 diabetes. , Journal of the American Pharmaceutical Association 53, 267-272.
- 20.Salas M, Hughes D, Zuluaga A, Vardeva K, Lebmeier M. (2009) Costs of medication nonadherence in patients with diabetes mellitus: a systematic review and critical analysis of the literature. , Value Health 12, 915-922.
- 21.Hu J, Wallace D, T P McCoy, K A Amirehsani. (2014) A family-based diabetes intervention for Hispanic adults and their family members.Diabetes Education,40,48-59.Care,37,S14-S80.
- 22.Robert Wood Johnson.Foundation (RWJF) & the University of Wisconsin Population Health Institute. (2012)Community health ranking: Mobilizing action toward community health. Retrieved from http://www.countyhealthrankings.org/texas/health-factors-rankings
- 23.Whittemore R. (2007) Culturally competent interventions for Hispanic adults with type 2 diabetes: A systematic review. , Journal of Transcultural Nursing 18, 157-166.
- 24.S M Asch, E A Kerr, Keesey J, J L Adams, C M Setodji et al. (2006) Who is at greatest risk for receiving poor-quality health care? New England. , Journal of Medcine 354, 1147-1156.
- 25.H F Kao, M R Lynn, Lujan J. (2010) Lessons learned in instrument pilot testing with Mexican American caregivers of elders. , Journal of Nursing Measurement 18, 201-209.
- 26.Moher D, Liberati A, Tetzlaff J, D G Altman. (2009) The PRISMA Group. , Open Medicine 3, 123-130.
- 27.S V Doubova, Mino-Leon D, Perez-Cuevas R. (2013) Linking quality of healthcare and health-related quality of life of patients with type 2 diabetes: an evaluative study in Mexican family practice. , Inernational Journal for Quality in Health Care 25, 664-672.
- 28.P M Trief, Grant W, Elbert K, R S Weinstock. (1998) Family environment, glycemic control, and the psychosocial adaptation of adults with diabetes. , Diabetes Care 21, 241-245.
- 29.Bauer A M, Schillinger D, Parker M M, Katon W, Adler N et al. (2013) Health literacy and antidepressant medication adherence among adults with diabetes: the diabetes study of Northern California (DISTANCE). , Journal of General Internal Medicine 28, 1181-1187.
- 30.HealthyPeoplegov. (2013) Healthy People 2020: Health Communication and health information technology.Retrieved from http://www.healthypeople.gov/2020/.
- 31.J A Pagan, C J Brown, D A Asch, Armstrong K, Bastida E et al. (2012) Health literacy and breast cancer screening among Mexican American women in South Texas. , Journal of Cancer Education 27, 132-137.
- 32.Hu J, Amirehsani K, D C Wallace, Letvak S. (2013) Perceptions of barriers in managing diabetes: perspectives of Hispanic immigrant patients and family members. , Diabetes Eduation 39, 494-503.
- 33.Rothman R, Malone R, Bryant B, Horlen C, DeWalt D et al. (2004) The relationship between literacy and glycemic control in a diabetes disease-management program. , Diabetes Education 30, 263-273.
- 34.C L Latham, Calvillo E. (2009) Predictors of successful diabetes management in low-income Hispanic people. , Western Journl of Nursing research 31, 364-38837.
- 35.R B Trivedi, Piette J, S D Fihn, Edelman D. (2012) Examining the interrelatedness of patient and spousal stress in heart failure: conceptual model and pilot data. , Journal of Cardiovascular Nursing 27, 24-32.
- 36.Gleeson-Kreig J, Bernal H, Woolley S. (2002) The role of social support in the self-management of diabetes mellitus among a Hispanic population. , Public Health Nursing 19, 215-222.
- 37.H F Kao, M R Lynn, An K. (2012) Measurement of expectations of family loyalty of children toward elderly relatives with Mexican Americans. , Journal of Theory Construction & Testing 16, 38-44.
- 38.U S BureauofCensusCensus. (2012) 2009-2011American Community survey 3-year estimates: Hispanic or Latino origin by specific origin- universe: total population.Retrieved from http://www.socialexplorer.com/data/ACS2011_3yr metadata/?ds=American+Community+Survey+Tables%3A+2009+--+2011+%283-Year+Estimates%29&table=C03001.
- 39.U S BureauofCensusCensus.. (2013).Fact Sheet:El Paso County,Texas.Retrieved fromhttp://quickfacts.census.gov/qfd/states/48/48141.html
- 40.J O Rivera, Ortiz M, Cardenas V. (2009) Cross-border purchase of medications and health care in a sample of residents of El Paso. , Texas, and Ciudad Juarez, Mexico, Journal of National Medicine Association 101, 167-173.
- 41.H F Kao, An K. (2012) The effects of acculturation and mutuality on expectations of family loyalty among Mexican-American family caregiver of older adults. , Journal of Nursing Scholarsip 44, 111-119.
- 42.Fanus K, Huddleston R, Wisotzkey S, Hempling R. (2014) Embracing a cultu of safety by decreasing medication errors. , Nursing Management 45, 16-19.
- 43.Corsonello A, Pedone C, Lattanzio F, Lucchetti M, Garasto S et al. (2009) Regimen complexity and medication nonadherence in elderly patients. , Therapeutic Clinical Risk Management 5, 209-216.
- 44.Tong G, Hua X, Zhong Y, Zhang K, Gu G et al. (2014) Intensive insulin therapy increases sex hormone-binding globulin in newly diagnosed type 2 diabetic patients. , European Journal of Endocrinology 170, 237-245.
- 45.Thorpe J M, Thorpe C T, Kennelty K A, Gellad W F, Schulz R. (2012) The impact of family caregivers on potentially inappropriate medication use in noninstitutionalized older adults with dementia. , American Journal of Geriatric Pharmacotherapy 10, 230-241.
- 46. (2000) National Academy on Aging Society. Diabetes: A drain on U.S. resources. Retrieved from http://www.agingsociety.org/agingsociety/pdf/diabetes.pdf
- 47.Holland R, Lenaghan E, Smith R, Lipp A, Christou M et al. (2010) Delivering a home-base medication review, process measure from the HOMER randomised controlled trial. , International Journal of Pharmacy Practice 14, 71-79.
- 48.N S Ahmad, Ramli A, Islahudin F, Paraidathathu T. (2013) Medication adherence in patients with type 2 diabetes mellitus treated at primary health clinics in Malaysia. Patient Preference and Adherence. 7, 525-530.
- 49.J S Hong, H C Kang. (2011) Relationship between oral antihyperglycemic medication adherence and hospitalization, mortality, and healthcare costs in adult ambulatory care patients with type 2 diabetes in South Korea. , Medical Care 49, 378-384.
- 50.Farmer F, A L Kinmonth, Sutton S. (2006) Measuring beliefs about taking hypoglycaemic medication among people with type 2 diabetes. , Diabetes Medicine 23, 265-270.
- 51. (2012) Office of Minority Health,DHHS. Hispanic/Latino profile. Retrieved from http://minorityhealth.hhs.gov/templates/browse.aspx?lvl=2&lvIID=54
- 52.Centers for (2010) Medicare & Medicaid Services Chronic Condition Data Warehouse. , New Orleans, LA
- 53.Jacobson S, F G Wood. (2004) Contributions of children to the care of adults with diabetes. , Diabetes Education 30, 820-826.
- 54.Kim H, Chang M, Rose K, Kim S. (2012) Predictors of caregiver burden in caregivers of individuals with dementia. , Journal of Advanced Nursing 68, 846-855.
- 55.McDonald M V, T R Peng, Sridharan S, J B Foust, Kogan P et al. (2013) Automating the medication regimen complexity index. , Journal of American Medical Informatics Association 20, 499-505.